,
18 tweets,
14 min read
Read on Twitter
#Tweetorial: Diagnosis of Malignant Pleural Effusion (#MPE) to accompany publication in @AnnalsATS: bit.ly/2XM65pD
⚓️#MPE: Pl. Effusions (#pleff) w/ neoplastic cells/tissue
⚓️Paramalignant eff: related to malignancy but not due to it eg: endobronchial obstruction or PE
⚓️#MPE: Pl. Effusions (#pleff) w/ neoplastic cells/tissue
⚓️Paramalignant eff: related to malignancy but not due to it eg: endobronchial obstruction or PE
Answer me this dear folks!
Why is it important to diagnose #MPE?
While you ponder, LUNG and BREAST are commonest primaries metastatic to the pleural space! PMID: 24360987
Why is it important to diagnose #MPE?
While you ponder, LUNG and BREAST are commonest primaries metastatic to the pleural space! PMID: 24360987


PET/CT you ask?
In TB endemic area, PET by itself had sens of 63% ONLY!
Why?
TB lights up too!
PET added to CT ↑ sensitivity 70% --> 93%! (PMID: 27560933)
Specificity is low (30ish%) because of false positives (doi:10.1148/radiol.12110872):
- s/p pleurodesis
- infection /TB
In TB endemic area, PET by itself had sens of 63% ONLY!
Why?
TB lights up too!
PET added to CT ↑ sensitivity 70% --> 93%! (PMID: 27560933)
Specificity is low (30ish%) because of false positives (doi:10.1148/radiol.12110872):
- s/p pleurodesis
- infection /TB

To summarize: Clinical and radio features ↑ suspicion for #MPE, but we still don't have a DIAGNOSIS (need cells or tissue!)
#thoracentesis + PF analysis is the next step!
#Trivia: “Cancer Ratio” = Sr. LDH / Pl. ADA >20 has sensitivity of 98% and specificity of 94% for #MPE!
#thoracentesis + PF analysis is the next step!
#Trivia: “Cancer Ratio” = Sr. LDH / Pl. ADA >20 has sensitivity of 98% and specificity of 94% for #MPE!
1st #pleff cytology: 51% yield --> ↑ only to 59% on 2nd (WOMP!)
📈Yields much higher for "exfoliative" cancers: Lung AdenoCa / Ovarian
👎Yields VERY low for "non-exfoliative": Squamous #LungCancer
So: repeat cyto if primary likely exfoliative, otherwise proceed to next step!
📈Yields much higher for "exfoliative" cancers: Lung AdenoCa / Ovarian
👎Yields VERY low for "non-exfoliative": Squamous #LungCancer
So: repeat cyto if primary likely exfoliative, otherwise proceed to next step!
I'm often asked, how much fluid should we send for cytology and for cell block?
What is your practice? Leave comments!
For those of you wanting to learn more about "exfoliative" aspects of malignancies: I recd this 1964 article by Dr. Naylor from @UMich!
bit.ly/2XOIBjR
What is your practice? Leave comments!
For those of you wanting to learn more about "exfoliative" aspects of malignancies: I recd this 1964 article by Dr. Naylor from @UMich!
bit.ly/2XOIBjR

But "non-exfoliative" malignancies, higher sens than #pleff cyto eg 47% for Squamous Lung Ca. Long story short, LIMITED ROLE so far for tumor markers, but keep an eye out, work is being done!
So! pleff cyto has failed you, what's next??
So! pleff cyto has failed you, what's next??
"Blind" biopsies: 40% yield for #MPE (because patchy pleural involvement): NOT advised!
Real time CT guided or POCUS guided #pleuralbiopsy is the next choice, depending on local availability (sens high 80%)!
NOTE: Sensitivity is higher if pleura >1 cm thick!
PMID: 25997433
Real time CT guided or POCUS guided #pleuralbiopsy is the next choice, depending on local availability (sens high 80%)!
NOTE: Sensitivity is higher if pleura >1 cm thick!
PMID: 25997433
And for #MPE still undiagnosed #Thoracoscopy is next!
VATS vs Medical Thoracoscopy (#MT): Surgeon vs Pulm (usually), GA vs Local +/- TIVA
Co-author @naj_rahman (PMID: 20696694): Very low mortality for #MT
Recent data (PMID:29577922) for VATS also shows improved risk profile!
VATS vs Medical Thoracoscopy (#MT): Surgeon vs Pulm (usually), GA vs Local +/- TIVA
Co-author @naj_rahman (PMID: 20696694): Very low mortality for #MT
Recent data (PMID:29577922) for VATS also shows improved risk profile!
Word to the wise:
Not every patient is capable of undergoing thoracoscopy, esp the GA and single lung ventilation need for VATS!
Some absolute contraind for #thoracoscopy:
🛑Lung extensively adherent to chest wall
🛑Resting hypercapnia, likely to worsen during/after procedure
Not every patient is capable of undergoing thoracoscopy, esp the GA and single lung ventilation need for VATS!
Some absolute contraind for #thoracoscopy:
🛑Lung extensively adherent to chest wall
🛑Resting hypercapnia, likely to worsen during/after procedure
The hardest part?
Upto 30% cytology and histology negative pleural effusions are not diagnosed and get labeled "non specific pleuritis".
Upto 12% OF THESE EVENTUALLY TURN OUT TO BE PLEURAL MALIGNANCY, SO PLEASE BE CLINICALLY VIGILANT W/ THESE PATIENTS!
(PMID: 27625443)
Upto 30% cytology and histology negative pleural effusions are not diagnosed and get labeled "non specific pleuritis".
Upto 12% OF THESE EVENTUALLY TURN OUT TO BE PLEURAL MALIGNANCY, SO PLEASE BE CLINICALLY VIGILANT W/ THESE PATIENTS!
(PMID: 27625443)
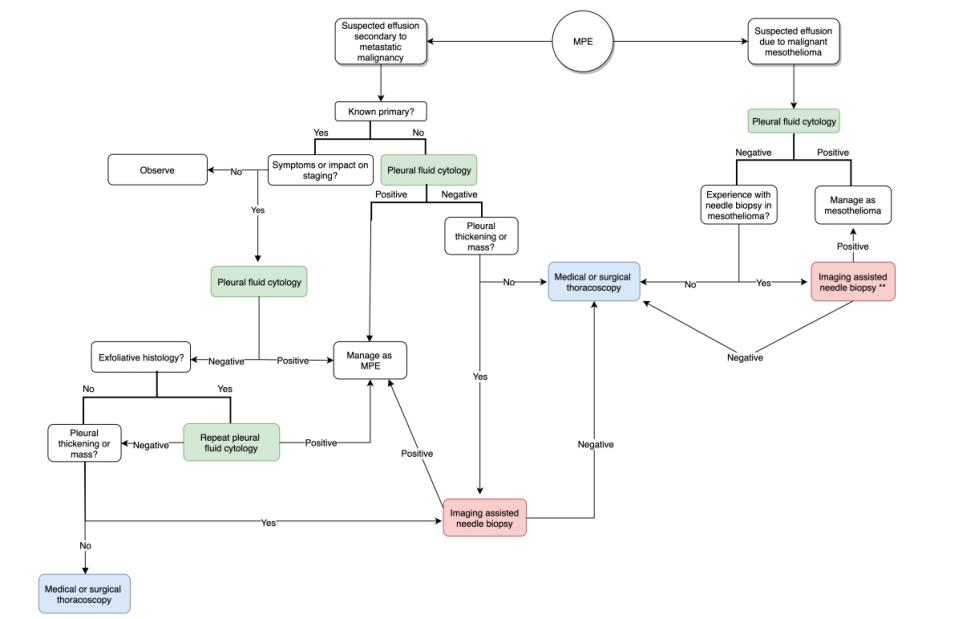
We advise this algorithmic approach to diagnosis of #MPE
In summary:
- Send 75 cc for cyto, 150 cc for cell block
- Repeat cyto for exfoliative types
- Proceed to imaging Bx or thoracoscopy per risk profile and local exp
- Stay vigilant if no diagnosis!
In summary:
- Send 75 cc for cyto, 150 cc for cell block
- Repeat cyto for exfoliative types
- Proceed to imaging Bx or thoracoscopy per risk profile and local exp
- Stay vigilant if no diagnosis!
Thanks for your comments #medtwitter, especially @rjhomer57: there is certainly room for more details on cyto-pathological nuances in diagnoses of #MPE!
Finally, thank you @GoodishIntent @ETSshow @laxswamy @hshanawaniMD for always encouraging me to be a better teacher!
Finally, thank you @GoodishIntent @ETSshow @laxswamy @hshanawaniMD for always encouraging me to be a better teacher!