,
17 tweets,
11 min read
Read on Twitter
OK #hospmed19, I had told myself I wasn't going to make another #tweetorial until next week to give myself a break, but I can't help but be motivated by all the amazing #tweeps at this meeting. Long story short, here's a #medthread on #PSORIASIS!
#MedEd #FOAMed PC:@dermnetnz
1/
#MedEd #FOAMed PC:@dermnetnz
1/
More and more, we are recognizing psoriasis to be a systemic disease. Aside from the psoriatic #arthritis we all know and love, there is more convincing evidence that psoriasis is linked with #cardiovascular disease and risk. As such, #multidisciplinary care is important!
2/
2/
There are many different variants of psoriasis. The most classic is plaque psoriasis, described commonly as "salmon colored plaques with micaceous scale."
Q: Ever notice how psoriasis doesn't really get impetiginized/superinfected but eczema does? Why do you think that is?
3/
Q: Ever notice how psoriasis doesn't really get impetiginized/superinfected but eczema does? Why do you think that is?
3/
Psoriasis is Th1>>Th2, leading to less superinfection! Note how these photos of plaque psoriasis don't have the "impetigo" look that eczema often does. Psoriasis is also "drier." The third photo is the histology of psoriasis. Note the vessels that reach near epidermis.
4/
4/


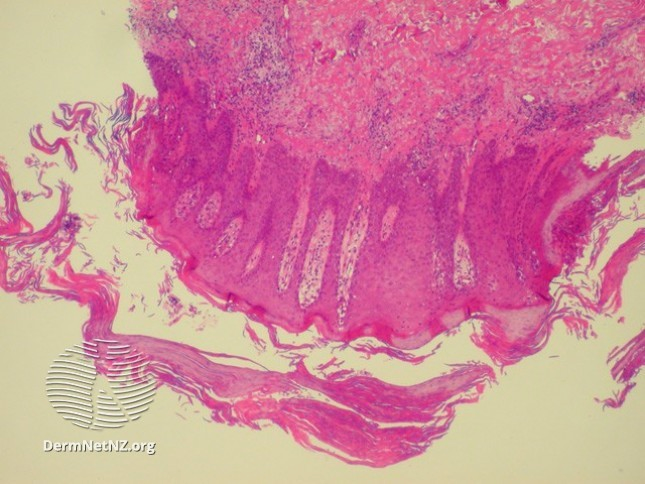
Those vessels correlate to the clinically relevant "Auspitz sign," where pulling a scale off the plaque will leave pinpoint bleeding underneath. I've always found this to be a really neat clinico-pathologic correlation!
5/
5/
Psoriasis can also look like complete erythroderma (redness over 80% of the body - photo 1), inverse psoriasis (just in the skin folds - photo 2), pustular psoriasis (lakes of pus and pustules over a red base - photo 3), and can be "guttate" or "drop like" (photo 4).
6/
6/




All these subtypes can have their own implications.
erythroderma - think about insensible fluid losses.
inverse - avoid high potency topical steroids given location.
pustular - can be ill w/fevers (Von Zumbusch type), & low Ca2+
guttate - often 2/2 strep throat! may need abx!
7/
erythroderma - think about insensible fluid losses.
inverse - avoid high potency topical steroids given location.
pustular - can be ill w/fevers (Von Zumbusch type), & low Ca2+
guttate - often 2/2 strep throat! may need abx!
7/
Remember that psoriasis can affect the hands & feet, as well as the groin! There's also a less common subtype of "acrodermatitis continua of hallopeau," where only the distal fingers are involved - and it can be pustular, causing the patient to lose their nails!
8/
8/


If you see a rash, and suspect psoriasis, there are certain areas to look to see if there are clues. These include:
- Nails
- Occipital scalp
- Superior gluteal cleft (just looks pink)
- umbilicus
Don't forget about the differences in psoriasis and eczema which can help.
9/
- Nails
- Occipital scalp
- Superior gluteal cleft (just looks pink)
- umbilicus
Don't forget about the differences in psoriasis and eczema which can help.
9/


About those nails, they usually can show the following:
- Oil drop spots
- onycholysis (nail lifting off nailbed)
- pitting (haphazard)
- leukonychia (white spots)
While you're looking at the hands, don't forget to ask about joint pain and consider a joint exam!
10/
- Oil drop spots
- onycholysis (nail lifting off nailbed)
- pitting (haphazard)
- leukonychia (white spots)
While you're looking at the hands, don't forget to ask about joint pain and consider a joint exam!
10/


Remember psoriatic arthritis is one of the seronegative spondyloarthritides (HLA-B27!). Like other inflammatory joint processes, patients usually have more pain in the AM that improves over the course of the day with use. This is a do not miss dx, as it can be mutilating!
11/
11/

But how do you treat psoriasis? If it's just skin & it's mild, topical steroids alternating with a vitamin D analogue (eg:calcipotriene) BID two weeks at a time is a good start. However, if there are concerns for systemic issues (eg: arthritis, CV risk), you may need more.
12/
12/
Before we get to systemics, phototherapy is also a good option for psoriasis. It doesn't help the joints or CV risk, but because it's skin directed, there aren't any systemic side effects to worry about. It can be pricey (2/2 copay) & annoying (TIW!). Some people love it!
13/
13/
If you're reaching for systemics, I'd suggest involving a #dermatologist or #rheumatologist to help. Methotrexate is good, but aside from helping peripheral arthritis & the skin, doesn't do much more than that. If you have axial/central arthritis, consider biologics.
14/
14/
The # of biologics for psoriasis is growing all the time! Most tried & true are the anti-TNFs. Ustekinumab, which targets IL-12 & IL-23 can be helpful too, & new in the last few years are the anti-IL17 & anti-IL23 drugs.
Anti-TNF are >> ustekinumab for CV risk mitigation.
15/
Anti-TNF are >> ustekinumab for CV risk mitigation.
15/
Oh, don't forget about #Koebner phenomenon! This is when epidermal injury causes the skin to re-create an inflammatory disorder at the site of injury! So when you see psoriasis in weird patterns, think about whether that may be the underlying reason! (photo 2 is 2/2 zoster!)
16/
16/


Apologies for the long tweetorial! Given the many implications psoriasis carries, I think it's an important disease to know a bit about. I'm sure that #dermtwitter and #rheumtwitter have more to add, so please do! Thanks for joining me!
#dermatology #medtwitter #derm
17/17
#dermatology #medtwitter #derm
17/17