Discover and read the best of Twitter Threads about #B2BPearl
Most recents (7)

@MondayNightIBD 1/ 📣 #GITwitter #IBDTwitter
It’s a new🔥#Back2Basics session with #GI #Fellow @JosephHabibi_MD
Let’s talk AZA/6-MP in IBD
✅#IBDPolls 1️⃣&2️⃣👆🏽
✅Role as Mono/combo therapy
✅Escalation consideration
✅TPMT & NUDT15 testing
✅Side effects & counseling
It’s a new🔥#Back2Basics session with #GI #Fellow @JosephHabibi_MD
Let’s talk AZA/6-MP in IBD
✅#IBDPolls 1️⃣&2️⃣👆🏽
✅Role as Mono/combo therapy
✅Escalation consideration
✅TPMT & NUDT15 testing
✅Side effects & counseling
@MondayNightIBD @NavreetChowlaMD @MilestoneIBD @IBD_FloMD @tinahamd @DrCoreySiegel @HorstIBDDoc @MLongMD @LauraRaffalsMD @doc_ibd @IBDBen 2/ AZA trials in IBD:
🔹Corticosteroids needed to induce remission
🔹Takes ~12 wks for AZA/6MP to become effective, so taper steroids accordingly
🔹AZA/6-MP effective for maintenance of remission (mainly in UC); Not effective for induction
🔹Corticosteroids needed to induce remission
🔹Takes ~12 wks for AZA/6MP to become effective, so taper steroids accordingly
🔹AZA/6-MP effective for maintenance of remission (mainly in UC); Not effective for induction


@MondayNightIBD @NavreetChowlaMD @MilestoneIBD @IBD_FloMD @tinahamd @DrCoreySiegel @HorstIBDDoc @MLongMD @LauraRaffalsMD @doc_ibd @IBDBen @IBDHorizons @IBD_Houston @IrisWangMD @LoriPlung @vaibhav_manu @KatieFalloonMD @amneethansmd @ManuelBragaMD @Chatterjee_MD @SuhaAbushamma 3/ AZA in today’s practice
1⃣CS-sparing monotherapy for maintenance of moderate IBD
2⃣Combo w/ TNFi to
↑ TNFi levels
↓ Ab formation
2nd MOA for severe/complex IBD not responsive to mono💉
Perianal Crohn’s
...⏬
1⃣CS-sparing monotherapy for maintenance of moderate IBD
2⃣Combo w/ TNFi to
↑ TNFi levels
↓ Ab formation
2nd MOA for severe/complex IBD not responsive to mono💉
Perianal Crohn’s
...⏬

@dunleavy_katie @MondayNightIBD @BattatMD4IBD @DCharabaty @JosephHabibi_MD @KanikaGargMD @Spencerkelley7 @BassiMehak @jalpa_devi @Empoweringpts9 @ayshaslam999 @RomyChamoun @JHaydek @BettenworthDb @MaiaKayalMD @IBD_FloMD @APandT @debby_keller @ibdseb @IBDJournals @ezzatali64 @PracUpGastro @TwittyWhitty22 @1yr @5yr @charlie_lees @P_DeepakIBDMD @EdwardLoftus2 @drvishal82 @guthealthmd @GuiRamosMD @MRegueiroMD @JanDabritz @MatthieuAllez @AmerGastroAssn @AGA_Gastro @ibdleuven @JeanFredericCo1 @SeverineVermei1 @GianlucaPellino @fgomollon @bverstockt @mchiorean4 @Gut_BMJ @BenClickMD @IBDcanruti @ASGEendoscopy @PeyrinBiroulet @BrunoSilva_MD @MatFume 7/⬆️the risk of POR❓
Patient factors:
💎👨>👸
💎 >15 🚬/day
💎Young age at the time of ✂️ (<30 y)
Disease &💊factors:
💎Short disease duration before ✂️
💎>2 prior ✂️
💎Penetrating disease
💎SB resection >50 cm
💎➕ disease at resection margin
💎➖of post✂️ anti-TNF therapy
Patient factors:
💎👨>👸
💎 >15 🚬/day
💎Young age at the time of ✂️ (<30 y)
Disease &💊factors:
💎Short disease duration before ✂️
💎>2 prior ✂️
💎Penetrating disease
💎SB resection >50 cm
💎➕ disease at resection margin
💎➖of post✂️ anti-TNF therapy

@dunleavy_katie @MondayNightIBD @BattatMD4IBD @DCharabaty @JosephHabibi_MD @KanikaGargMD @Spencerkelley7 @BassiMehak @jalpa_devi @Empoweringpts9 @ayshaslam999 @RomyChamoun @JHaydek @BettenworthDb @MaiaKayalMD @IBD_FloMD @APandT @debby_keller @ibdseb @IBDJournals @ezzatali64 @PracUpGastro @TwittyWhitty22 @1yr @5yr @charlie_lees @P_DeepakIBDMD @EdwardLoftus2 @drvishal82 @guthealthmd @GuiRamosMD @MRegueiroMD @JanDabritz @MatthieuAllez @AmerGastroAssn @AGA_Gastro @ibdleuven @JeanFredericCo1 @SeverineVermei1 @GianlucaPellino @fgomollon @bverstockt @mchiorean4 @Gut_BMJ @BenClickMD @IBDcanruti @ASGEendoscopy @PeyrinBiroulet @BrunoSilva_MD @MatFume 8/⬇️the risk of POR❓
🧬Older patient (>50 y)
🧬Nonsmoker
🧬1st Sx for a short segment of fibrostenotic disease (<10 to 20 cm)
#B2BPearl #MondayNightIBD No difference in recurrence between Eastern and Western countries‼️
Take a look!
pubmed.ncbi.nlm.nih.gov/30126030/
🧬Older patient (>50 y)
🧬Nonsmoker
🧬1st Sx for a short segment of fibrostenotic disease (<10 to 20 cm)
#B2BPearl #MondayNightIBD No difference in recurrence between Eastern and Western countries‼️
Take a look!
pubmed.ncbi.nlm.nih.gov/30126030/
@dunleavy_katie @MondayNightIBD @BattatMD4IBD @DCharabaty @JosephHabibi_MD @KanikaGargMD @Spencerkelley7 @BassiMehak @jalpa_devi @Empoweringpts9 @ayshaslam999 @RomyChamoun @JHaydek @BettenworthDb @MaiaKayalMD @IBD_FloMD @APandT @debby_keller @ibdseb @IBDJournals @ezzatali64 @PracUpGastro @TwittyWhitty22 @1yr @5yr @charlie_lees @P_DeepakIBDMD @EdwardLoftus2 @drvishal82 @guthealthmd @GuiRamosMD @MRegueiroMD @JanDabritz @MatthieuAllez @AmerGastroAssn @AGA_Gastro @ibdleuven @JeanFredericCo1 @SeverineVermei1 @GianlucaPellino @fgomollon @bverstockt @mchiorean4 @Gut_BMJ @BenClickMD @IBDcanruti @ASGEendoscopy @PeyrinBiroulet @BrunoSilva_MD @MatFume 9/💎How to⬇️ POR risk?💊✂️
#B2BPearl Risk stratify pt & manage accordingly
💊Post-op
👉Nitroimidazole x3mos, if low risk
👉TNFi, start wk4, if high risk
✂️Kono-S anastomosis + extended mesenteric resection
🔦CLN at 6mos, adjust Rx per Rutgeerts score
pubmed.ncbi.nlm.nih.gov/34977147/
#B2BPearl Risk stratify pt & manage accordingly
💊Post-op
👉Nitroimidazole x3mos, if low risk
👉TNFi, start wk4, if high risk
✂️Kono-S anastomosis + extended mesenteric resection
🔦CLN at 6mos, adjust Rx per Rutgeerts score
pubmed.ncbi.nlm.nih.gov/34977147/

@yaransarkis @MondayNightIBD @AmerGastroAssn @Spencerkelley7 @ayshaslam999 @jalpa_devi @purnie_mae @dunleavy_katie @KanikaGargMD @MarcelYibirin @JHaydek @DCharabaty @mjayoushe @AmCollegeGastro @ASGEendoscopy @Realcecum 8/ What’s in a C-scope ?
💎 #B2BPearl💎New guidelines @AmerGastroAssn
🔹Use High Def scope+++
🔹HDef scope ➕ Chromo (dye spray or virtual) if h/o dysplasia
🔹If using Standard Def: SD scope ➕Chromo dye spray only (not virtual)
🔗journals.lww.com/ajg/Abstract/2…
💎 #B2BPearl💎New guidelines @AmerGastroAssn
🔹Use High Def scope+++
🔹HDef scope ➕ Chromo (dye spray or virtual) if h/o dysplasia
🔹If using Standard Def: SD scope ➕Chromo dye spray only (not virtual)
🔗journals.lww.com/ajg/Abstract/2…
@yaransarkis @MondayNightIBD @AmerGastroAssn @Spencerkelley7 @ayshaslam999 @jalpa_devi @purnie_mae @dunleavy_katie @KanikaGargMD @MarcelYibirin @JHaydek @DCharabaty @mjayoushe @AmCollegeGastro @ASGEendoscopy @Realcecum 9/ What to biopsy ?
➕Targeted Bx🎯 of abnormal mucosa
➕Resection of polypoid lesion
➕Random Bx to document histologic extent/ healing
➕Extensive Random 4 quadrant bx every 10 cm IF no chromo, h/o dysplasia, poor visualization, PSC, foreshortened colon
➕Targeted Bx🎯 of abnormal mucosa
➕Resection of polypoid lesion
➕Random Bx to document histologic extent/ healing
➕Extensive Random 4 quadrant bx every 10 cm IF no chromo, h/o dysplasia, poor visualization, PSC, foreshortened colon
@yaransarkis @MondayNightIBD @AmerGastroAssn @Spencerkelley7 @ayshaslam999 @jalpa_devi @purnie_mae @dunleavy_katie @KanikaGargMD @MarcelYibirin @JHaydek @DCharabaty @mjayoushe @AmCollegeGastro @ASGEendoscopy @Realcecum 10/ What’s next after dx of Invisible dysplasia ?
💎 #B2BPearl💎
🔹Invisible dysplasia
→ Get 2nd opinion from expert #GIPath
→ HD CLN + dye chromo by expert endoscopist + Extensive non-targeted Bx if no resectable lesion seen
💎 #B2BPearl💎
🔹Invisible dysplasia
→ Get 2nd opinion from expert #GIPath
→ HD CLN + dye chromo by expert endoscopist + Extensive non-targeted Bx if no resectable lesion seen

@MondayNightIBD @DCharabaty 1/ Thiopurines are associated with an increased risk of NMSC (non-melanoma skin cancer)
Which of the following is true about this risk relative to non-exposed IBD pts, duration of thiopurine use , and after thiopurine cessation 🛑#Back2Basics #MondayNightIBD
Which of the following is true about this risk relative to non-exposed IBD pts, duration of thiopurine use , and after thiopurine cessation 🛑#Back2Basics #MondayNightIBD
@MondayNightIBD @DCharabaty 32 y/o M with UC here for f/u. In remission x7 yrs on AZA 75mg/d. He is here to discuss his concerns about his risk of lymphoma associated w/ AZA. (HSTCL= hepatosplenic T cell; EBV-L= EBV assoc lymphoma) Which statement is true?
#Back2Basics #MondayNightIBD
#Back2Basics #MondayNightIBD
@MondayNightIBD @DCharabaty 2/ ‼️Cancer risk in IBD‼️can be→
🔺Disease related (eg CRC, anal CA)
🔺Therapy related ( Skin, Lymphoma, Cervical, Anal)
🔺Disease related (eg CRC, anal CA)
🔺Therapy related ( Skin, Lymphoma, Cervical, Anal)
@MondayNightIBD @SobiaMujtabaMD @NabilQuraishi @CholestasisDoc @DCharabaty 1/ 35 y/o M presents with fatigue & generalized pruritus x 6weeks. No skin rash, No abdo pain, diarrhea or 🩸 in stool. AST 62 ALT 64 ALP 435 Tbili 1.3. MRI/MRCP: multifocal strictures & areas of dilatation of intra +extra hepatic ducts. What’s the next step?💡 #Back2Basics #B2B
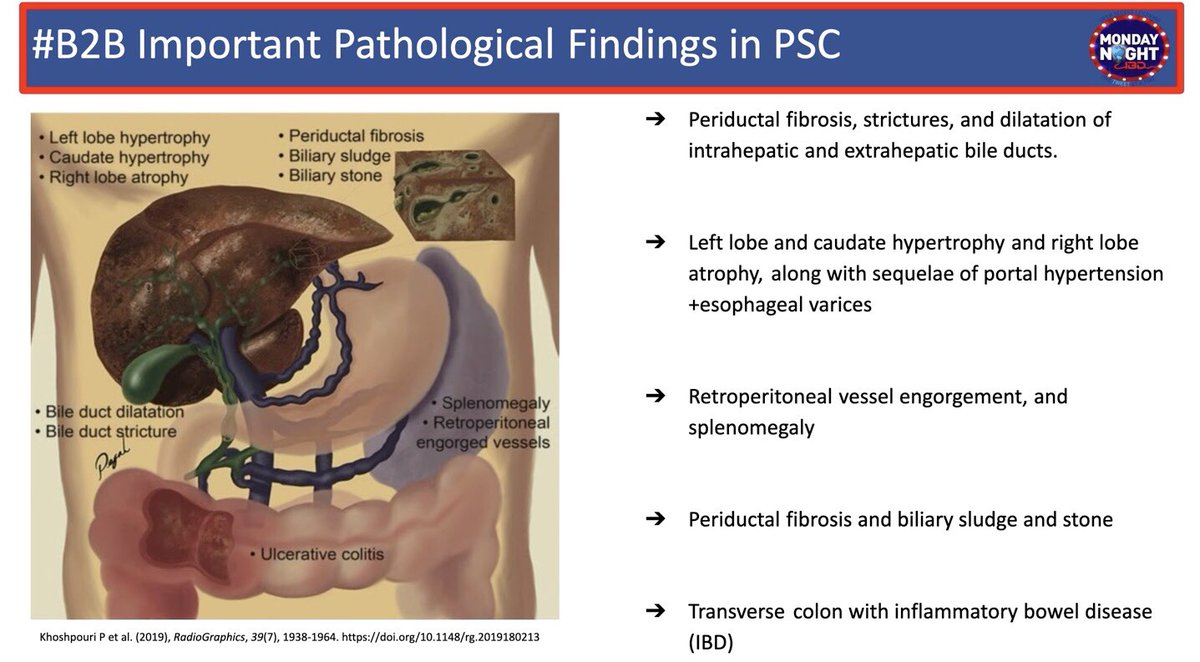
@MondayNightIBD @SobiaMujtabaMD @NabilQuraishi @CholestasisDoc @DCharabaty 2/ What’s #PSC & phenotypes?
🧩Idiopathic chronic inflam dis. of the biliary tree
🧩90%: Large ducts (LD): "Beads on string appearance” on ERCP/MRCP (pt👆)
🧩5% Small IHD only: nml MRCP, dx by liver bx, slide👇
🧩5% PSC w AIH overlap: abnl MRCP+liver bx w⬆️AST/ALT or IgG
🧩Idiopathic chronic inflam dis. of the biliary tree
🧩90%: Large ducts (LD): "Beads on string appearance” on ERCP/MRCP (pt👆)
🧩5% Small IHD only: nml MRCP, dx by liver bx, slide👇
🧩5% PSC w AIH overlap: abnl MRCP+liver bx w⬆️AST/ALT or IgG

@MondayNightIBD @SobiaMujtabaMD @NabilQuraishi @CholestasisDoc @DCharabaty 3/ 💎#B2BPearl #PSC w ⬆️IgG4
📌15% of LD-PSC
📌⬆️IgG4 serum>140mg/dL +/- tissue
💎✅IgG4 at least once w PSC dx
📌Assoc. w AI pancreatitis; other Ig4 dis.
💎⬆️severity of UC, colectomy
📌More rapid progression to cirhhosis
💎Steroid responsive: ️ ⬇️AlPhos, TBili, IgG4
📌15% of LD-PSC
📌⬆️IgG4 serum>140mg/dL +/- tissue
💎✅IgG4 at least once w PSC dx
📌Assoc. w AI pancreatitis; other Ig4 dis.
💎⬆️severity of UC, colectomy
📌More rapid progression to cirhhosis
💎Steroid responsive: ️ ⬇️AlPhos, TBili, IgG4
@MondayNightIBD @SobiaMujtabaMD @SchwartzbergMD @DCharabaty 1/ 27 yo F, crohns colitis on AZA, presents w 2wk perianal pain. One week ago a “boil” developed adjacent to the anus, painful to touch and draining cloudy fluid. PE: Perianal fistulous opening tender & draining pus on palpation. What is the next best step ? #B2B
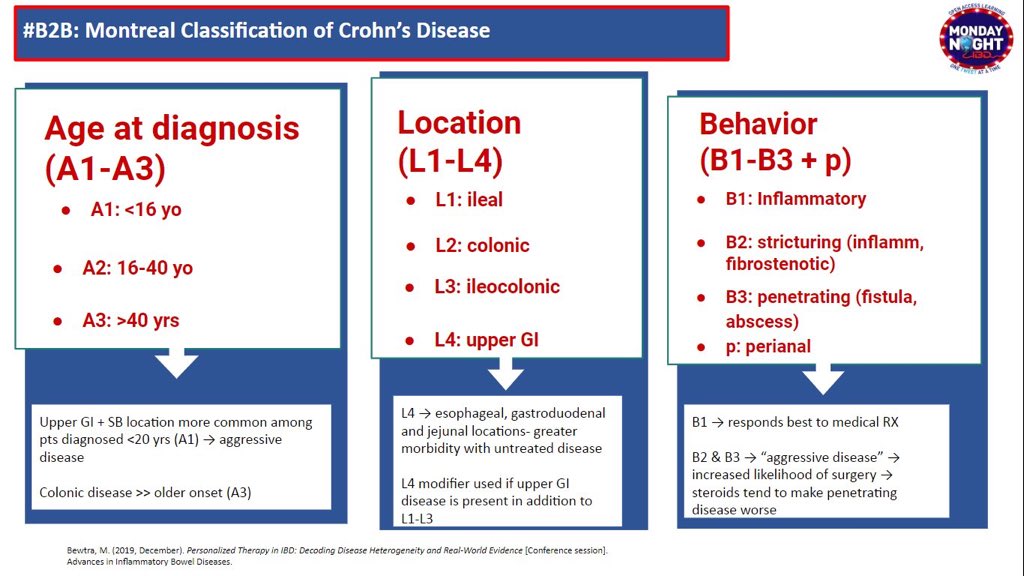
@MondayNightIBD @SobiaMujtabaMD @SchwartzbergMD @DCharabaty 2/Recap #Crohns:
📌Transmural inflammation involving any part of GIT
📌B for Phenotypes: inflammatory/stricturing/penetrating
📌L for location: UGI,SB,Colon
📌Penetrating Behaviors:
Fistulae
Perforations
Intra-abdominal abscesses(IAA)
recall this #B2B MTL classification table👇🏼
📌Transmural inflammation involving any part of GIT
📌B for Phenotypes: inflammatory/stricturing/penetrating
📌L for location: UGI,SB,Colon
📌Penetrating Behaviors:
Fistulae
Perforations
Intra-abdominal abscesses(IAA)
recall this #B2B MTL classification table👇🏼
@MondayNightIBD @SobiaMujtabaMD @SchwartzbergMD @DCharabaty 3/♦️p->Perianal ds in CD
♦️Can occur w any B&L
♦️May be initial manif in ~10%
♦️Can be isolated(no luminal dis)
♦️Affect up to 1/3 of CD pts
♦️Incidence cld be ⬇️w⬆️use of biologics @sang_hyoung @EdwardLoftus2 pubmed.ncbi.nlm.nih.gov/30346531/
♦️One of most challenging manif for pts+MDs
♦️Can occur w any B&L
♦️May be initial manif in ~10%
♦️Can be isolated(no luminal dis)
♦️Affect up to 1/3 of CD pts
♦️Incidence cld be ⬇️w⬆️use of biologics @sang_hyoung @EdwardLoftus2 pubmed.ncbi.nlm.nih.gov/30346531/
♦️One of most challenging manif for pts+MDs
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 25y/oM quit🚬3 mos ago, now 3🩸loose BM/day,mild abdo cramps;Cousin w Crohns;Stool➖for infection;CLN: erythematous granular mucosa rectum+sigmoid, superficial ulcers;BX:Acute cryptitis,crypt abscess,crypt architecture distortion. What helps most dx UC vs Crohn’s?
#B2B #IBDPoll
#B2B #IBDPoll
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty UC and CD:
🔻Chronic inflammation of the GI tract
🔻Affects all ages: Typically starts between age 20-39
🔻Second peak of incidence age >50
🔻Flares of GI symptoms +/-systemic symptoms +/- EIM
🔻Chronic inflammation of the GI tract
🔻Affects all ages: Typically starts between age 20-39
🔻Second peak of incidence age >50
🔻Flares of GI symptoms +/-systemic symptoms +/- EIM
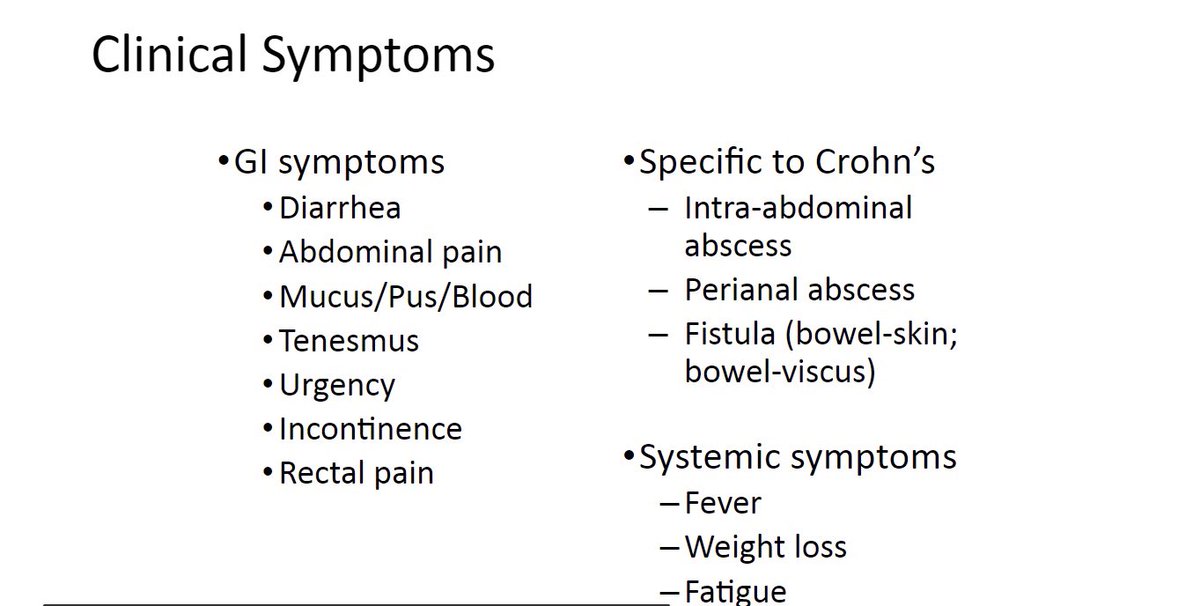
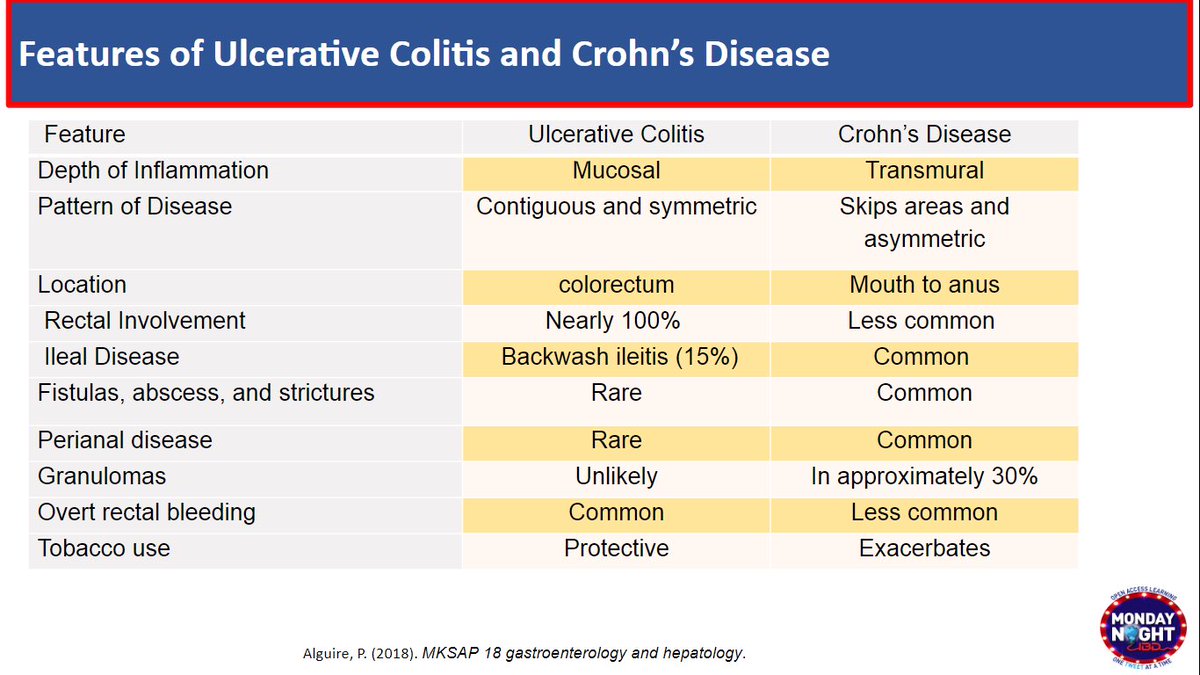
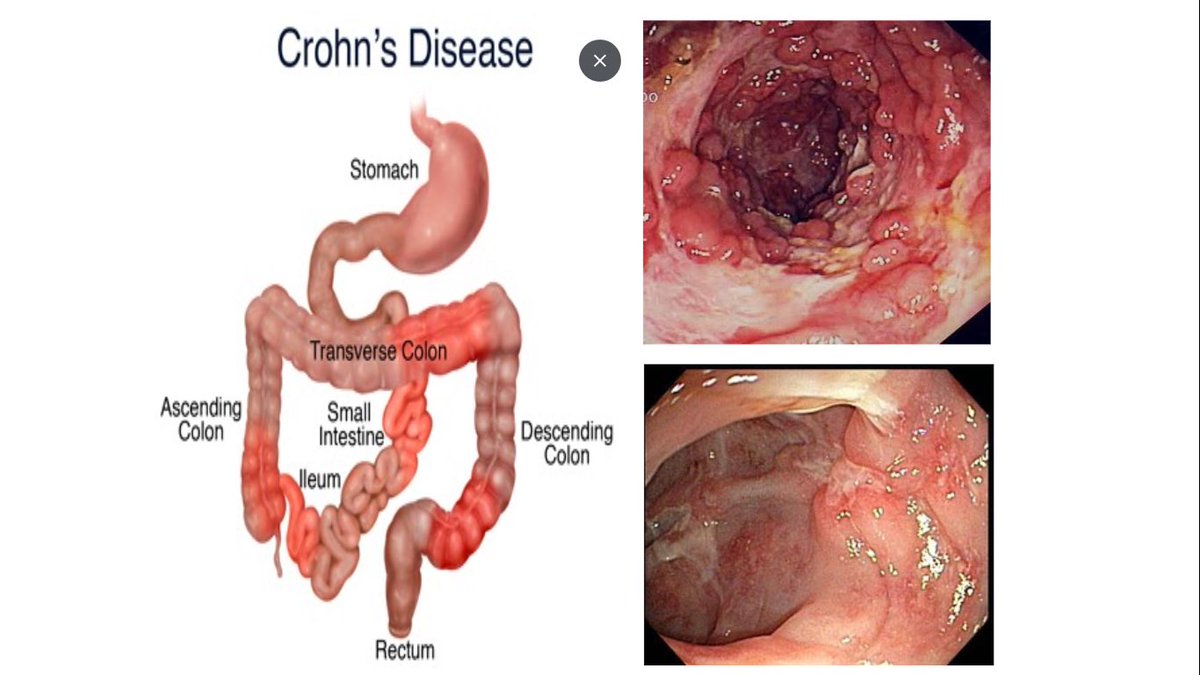
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 3/ CD:
💡Skipped lesion, any part of GI tract
💡Most common:Colon+ileum
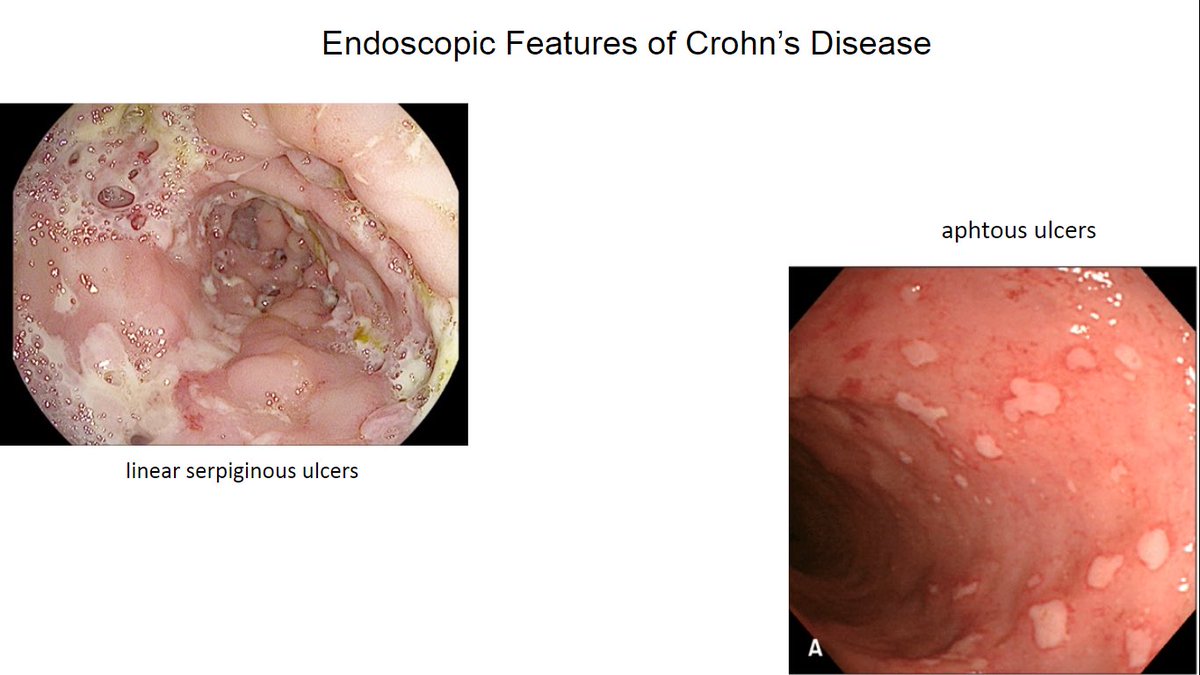
Hallmark➡️ulcers: aphthous,deep large/linear/serpiginous
💡Transmural inflamm -> stricturing, perforating dis.
🚩#B2BPearl
👉🏼Rectum can be involved in CD;➕anorectal ulcers → ⬆️risk of perianal disease
💡Skipped lesion, any part of GI tract
💡Most common:Colon+ileum
Hallmark➡️ulcers: aphthous,deep large/linear/serpiginous
💡Transmural inflamm -> stricturing, perforating dis.
🚩#B2BPearl
👉🏼Rectum can be involved in CD;➕anorectal ulcers → ⬆️risk of perianal disease