Discover and read the best of Twitter Threads about #ESMO22
Most recents (21)

@TumorBoardTues 1/17 #TumorBoardTuesday #RenalCancer #OncTwitter
68yo👨🏾
HTN
T2DM
Arthritis
✂️2022: L Radical Nephrectomy
🔬Clear cell #RenalCellCarcinoma
📏8.2 cm, Grade 2, extends into renal vein (T3a)
❓No lymph nodes sampled (NX)
❌No other dz sites
What would you pick for adj therapy?
68yo👨🏾
HTN
T2DM
Arthritis
✂️2022: L Radical Nephrectomy
🔬Clear cell #RenalCellCarcinoma
📏8.2 cm, Grade 2, extends into renal vein (T3a)
❓No lymph nodes sampled (NX)
❌No other dz sites
What would you pick for adj therapy?
@TumorBoardTues 2/17 #TumorBoardTuesday #RCC
🚨There’s significant relapse risk in ≥ Stage II RCC even after local tx✂️
🔢We use tools like Fox Chase’s ASSURE Prognostic nomogram to estimate disease free survival (DFS)
📈Example for our pt below
📚Correa, Andres F cancernomograms.com/nomograms/492
🚨There’s significant relapse risk in ≥ Stage II RCC even after local tx✂️
🔢We use tools like Fox Chase’s ASSURE Prognostic nomogram to estimate disease free survival (DFS)
📈Example for our pt below
📚Correa, Andres F cancernomograms.com/nomograms/492

@TumorBoardTues 3/17 #TumorBoardTuesday @brian_rini
⭐RCC Adjuvant Therapy⭐
⚖️Weighing recurrence risk with a long list 📜 of adj trial results?
💉Focusing on adju IO & review:
✨KEYNOTE-564: Pembro
✨CheckMate 914: Nivo/Ipi
✨IMmotion010: Atezo
✨PROSPER: Periop Nivo
⭐RCC Adjuvant Therapy⭐
⚖️Weighing recurrence risk with a long list 📜 of adj trial results?
💉Focusing on adju IO & review:
✨KEYNOTE-564: Pembro
✨CheckMate 914: Nivo/Ipi
✨IMmotion010: Atezo
✨PROSPER: Periop Nivo

1/22 #TumorBoardTuesday #OncTwitter
60yo 👩🏻
ER+/PR-/HER2 low met #BreastCancer
Since 2016: 3 lines of endocrine therapy including AI+CDK 4/6 inhibitor ➡️ Fulvestrant ➡️ Everolimus+exemestane
No actionable mutation
🤨 What would be your first chemotherapy choice:
60yo 👩🏻
ER+/PR-/HER2 low met #BreastCancer
Since 2016: 3 lines of endocrine therapy including AI+CDK 4/6 inhibitor ➡️ Fulvestrant ➡️ Everolimus+exemestane
No actionable mutation
🤨 What would be your first chemotherapy choice:
2/22 #TumorBoardTuesday @MPishvaian @JohnEbbenMDPhD #BreastCancer #BCSM
2021*: Started on capecitabine for 8 months until POD
2022: Switched to paclitaxel for 5 months ➡️ POD in the liver and pleura
🤨 What would be your next step?
2021*: Started on capecitabine for 8 months until POD
2022: Switched to paclitaxel for 5 months ➡️ POD in the liver and pleura
🤨 What would be your next step?
3/22 #TumorBoardTuesday
👩🏻🏫Mini tweetorial 1
📌What is HER2-low?
🔸Traditionally HER2-positive and HER2-negative were separate entities
🔸NOW, HER2-low is a separate entity 👉🏽 1+ or 2+ on IHC and ISH negative‼️
📚@PTarantinoMD @curijoey @stolaney1 aacrjournals.org/cancerdiscover…
👩🏻🏫Mini tweetorial 1
📌What is HER2-low?
🔸Traditionally HER2-positive and HER2-negative were separate entities
🔸NOW, HER2-low is a separate entity 👉🏽 1+ or 2+ on IHC and ISH negative‼️
📚@PTarantinoMD @curijoey @stolaney1 aacrjournals.org/cancerdiscover…

Dr. @ZPiotrowskaMD presents initial results from the ELIOS trial at #ESMO22 - molecular profiling of #EGFR mutant NSCLC after progression on 1L osimertinib.


In this study of highly motivated pts at esteemed sites, evaluable paired biopsy at PD only available in 46/115 pts (40%). Interestingly, 75 pts (65%) had paired biopsy but 27 failed NGS (23%). Speaks somewhat to the real world feasibility of a repeat biopsy approach. #ESMO22

Common co-mutations at baseline included TP53, EGFR amp, and CDKN2A loss. Acquired alterations included MET amp, EGFR C797S, ALK fusion, NKX2-1 amp. Mostly mutually exclusive. #ESMO22




1/n
I'm looking at $LPTX right now and trying to understand the stock price drop following #ESMO22.
There is actually little change in the data compared to previous ASCO-GI 2022 data.
If you do a more rigorous evaluation on an ITT basis and count only confirmed responses,
I'm looking at $LPTX right now and trying to understand the stock price drop following #ESMO22.
There is actually little change in the data compared to previous ASCO-GI 2022 data.
If you do a more rigorous evaluation on an ITT basis and count only confirmed responses,
2/n
the ORR is 52% and is not much greater than the ORR of nivo + chemo (47%) or tisle + chemo (47%). However, the mPFS is significantly greater (11.3 mo vs 7.7 mo and 6.1 mo, resp.). mOS has not been reached after a median study duration of 15.7 mo (nivo + chemo mOS =13.8 mo).
the ORR is 52% and is not much greater than the ORR of nivo + chemo (47%) or tisle + chemo (47%). However, the mPFS is significantly greater (11.3 mo vs 7.7 mo and 6.1 mo, resp.). mOS has not been reached after a median study duration of 15.7 mo (nivo + chemo mOS =13.8 mo).
3/n
Subgroup analysis is too complicated for a Twitter posting because of different, sometimes opposing influences, but does not change the summary.
Perhaps it irritated the investors that mPFS of DKK-high group (11.3 mo) is smaller than the mPFS of the DKK-low group (12.0 mo).
Subgroup analysis is too complicated for a Twitter posting because of different, sometimes opposing influences, but does not change the summary.
Perhaps it irritated the investors that mPFS of DKK-high group (11.3 mo) is smaller than the mPFS of the DKK-low group (12.0 mo).

#ESMO22 final Presidential Symposium III presentation, #IPSOS, evaluating atezolizumab vs single-agent chemotherapy in pts with advanced NSCLC unsuitable for 1L standard platinum-based chemotherapy, N=453, primary EP: OS






#ESMO22 Presidential Symposium III continued with the eagerly awaited #CodeBreak200 evaluating sotorasib vs docetaxel in pts w/ locally advanced or metastatic KRAS G12C-mutated NSCLC (N=345) presented by @MLJohnsonMD2 from @SarahCannonDocs

#ESMO22 #CodeBreak200 met it's primary EP of improved PFS by BICR with a median f/u of 17.7 mo. Median PFS: 5.6 vs 4.5 mo, HR=0.66, P=.002


#ESMO22 #CodeBreak200 ORR was higher in pts treated with sotorasib (28.1 vs 13.2%) and mDOR was longer with sotorasib (8.6 vs 6.8 mo). There was no difference in OS



#ESMO22 COSMIC-313 presented by @DrChoueiri Triplet therapy with cabo/nivo/ipi vs cabo/nivo for patients with advanced TN advanced intermediate or poor-risk #RCC. Primary EP: PFS; N=855

#ESMO22 #COSMIC313: Longer PFS with triplet vs doublet. mPFS NR vs 11.3 mo with benefit seen in most predefined subgroups #RCC





1/n
#ESMO22
▪ ZW49 $ZYME seems well tolerated, however, unexpected is the alopecia (→ the linker would need a closer look).
▪ The dose needs to be increased (T-DXd is dosed much higher).
▪ The efficacy data (ORR, DCR) at 2.5 mg/kg 3QW in ≥ 3L mBC are very weak,
#ESMO22
▪ ZW49 $ZYME seems well tolerated, however, unexpected is the alopecia (→ the linker would need a closer look).
▪ The dose needs to be increased (T-DXd is dosed much higher).
▪ The efficacy data (ORR, DCR) at 2.5 mg/kg 3QW in ≥ 3L mBC are very weak,
2/n
but those in ≥ 2L GEA are surprisingly about as good as T-DXd at 6.4 mg/kg 3QW.
▪After 3 years of phase 1, the overall data situation is very thin.
but those in ≥ 2L GEA are surprisingly about as good as T-DXd at 6.4 mg/kg 3QW.
▪After 3 years of phase 1, the overall data situation is very thin.
3/n
After reading through the transcript of the CC, I cannot understand the $ZYME Mgtm's rationale for moving ZW49 forward.
For example, in the 3L mBC indication, 1.5 mg/kg 3QW ARX788 $AMAM achieves 66% ORR and 5.4 mg/kg T-DXd $AZN achieves 61% (median 6 pretreatments in each
After reading through the transcript of the CC, I cannot understand the $ZYME Mgtm's rationale for moving ZW49 forward.
For example, in the 3L mBC indication, 1.5 mg/kg 3QW ARX788 $AMAM achieves 66% ORR and 5.4 mg/kg T-DXd $AZN achieves 61% (median 6 pretreatments in each

L'inquinamento atmosferico può causare il cancro ai polmoni nelle persone che non hanno mai fumato? Com'è possibile? C'è un nuovo meccanismo biologico/molecolare alla base. Un thread (lungo ma spero interessante) per parlarvene 1/n 🧵

Sì, è stato identificato un nuovo meccanismo attraverso il quale particelle inquinanti molto piccole nell'aria possono innescare cancro ai polmoni in persone che non hanno mai fumato, aprendo la strada a nuovi approcci di prevenzione e sviluppo di terapie da #ESMO22. 2/n
Si tratta di uno studio realizzato dagli scienziati del Francis Crick Institute, in particolare dal prof. Charles Swanton e dal suo team insieme all'University College di Londra. Parliamone. 3/n
Dr. Silvia Novello presents 5y update on KEYNOTE 407 (platinum plus tax and +/- pembrolizumab for 1L squamous NSCLC #ESMO22

With longer follow up, OS favors pembrolizumab arm with mOS 17.2 vs 11.6m (OS HR 0.71) in squamous NSCLC. 5y OS rate 18.4% vs 9.7%. PFS benefit (HR 0.62) and higher RR across PDL1 strata. #ESMO22




For patients who complete 2y of pembrolizumab, 3y OS rate (after completing 2y pembro) was 70% - though not all of those patients are cured (44% were alive without PD or subsequent therapy). #ESMO22

Dr. @marinagarassino presents 5-year efficacy and safety update of KEYNOTE-189 (1L carboplatin plus pemetrexed +- pembrolizumab in non-squamous NSCLC) #ESMO22

KEYNOTE 189 is our SOC and has shown a consistent benefit including improving OS even with a crossover rate of 57%. #ESMO22
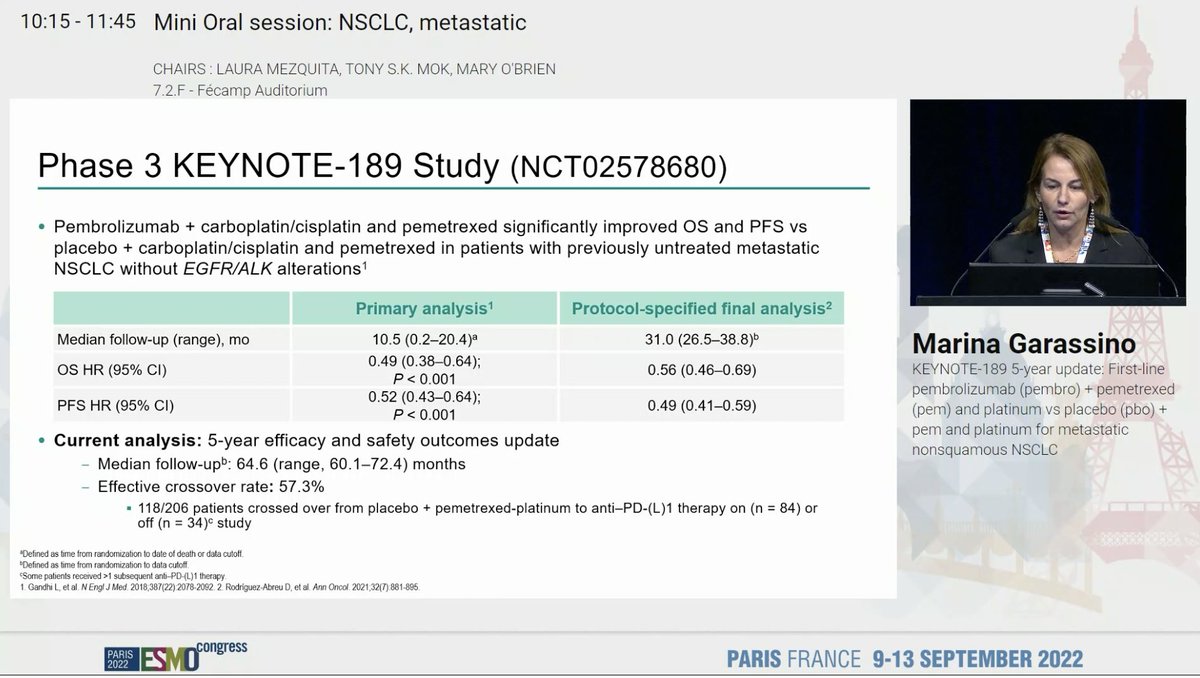
KEYNOTE 189 shows sustained OS benefit with longer follow up and a 5y OS rate of 18.4% with an OS HR of 0.60. Better PFS and OS also observed. Benefit across PDL1 strata. No new safety signals . #ESMO22




Dr. Baohui Han presents SUNRISE: randomized phase II study of sintilimab (PD1) and anlotinib (anti-angiogenic TKI) in metastatic NSCLC. #ESMO22

Study design here shows randomization to first-line sintilimab + anlotinib or chemo (with sintilimab at progression). Some concerns about randomization to chemotherapy without immunotherapy in a modern day study. #ESMO22


Baseline characteristics show a fairly high proportion of never smokers. SUNRISE excluded EGFR, ALK, and ROS1 - would like details on testing methods and presence of other drivers. More pts with brain and liver metastases in the sintilimab + anlotinib arm. #ESMO22





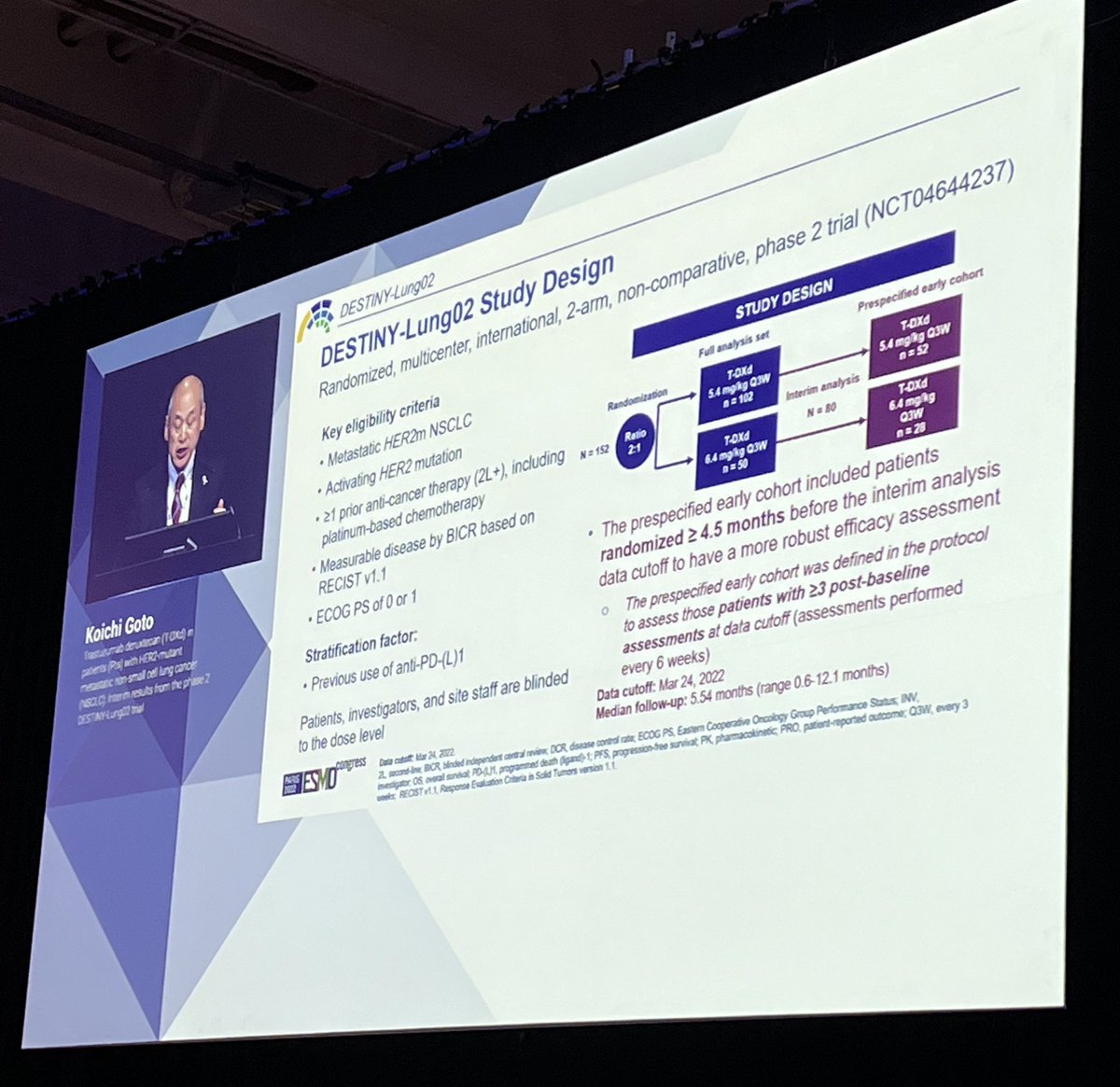
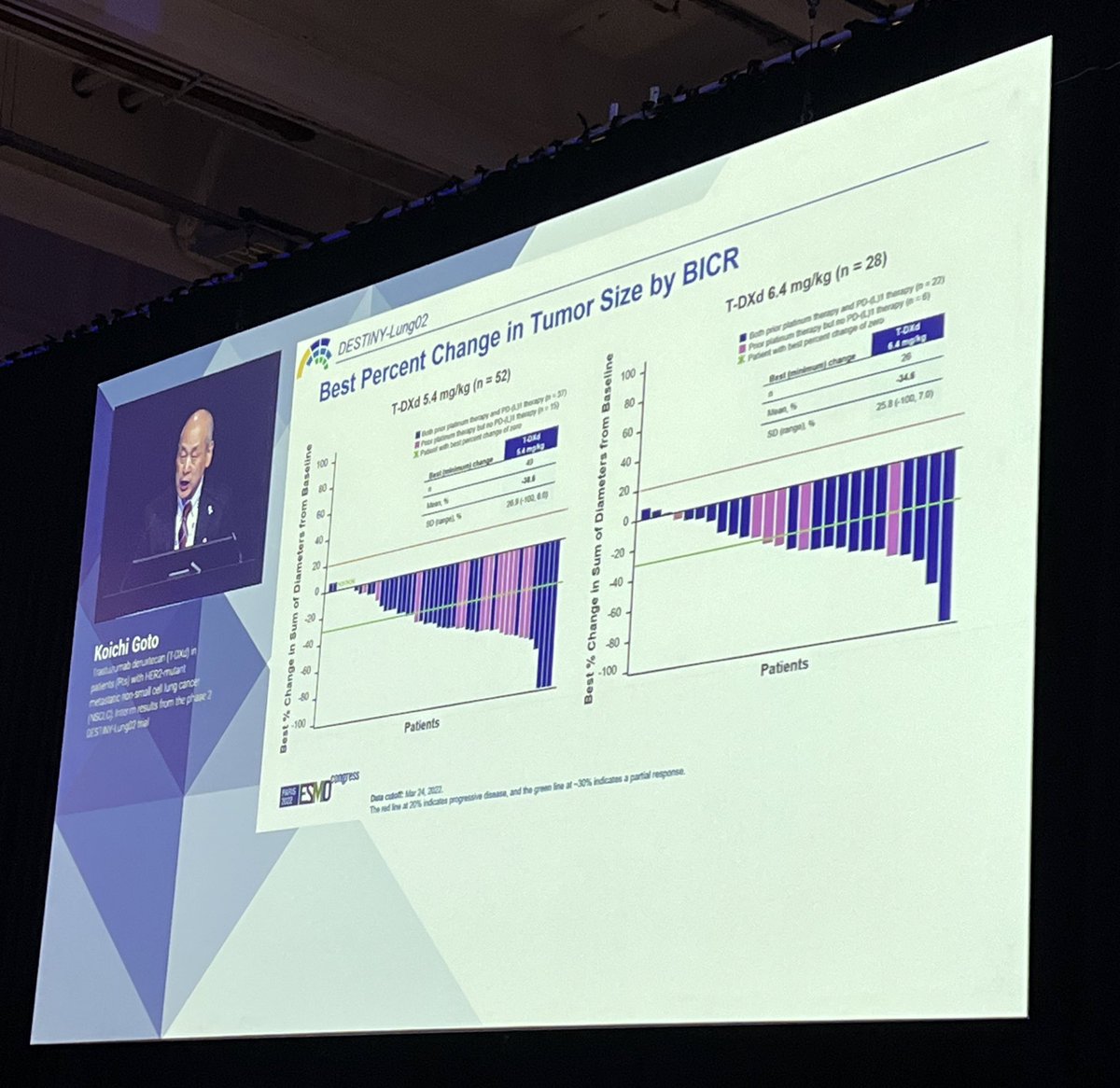
Dr. Koichi Goto starts the lung mini oral session with results from DESTINY-Lung02 of the recently approved trastuzumab deruxtecan in #HER2 NSCLC #ESMO22






Discussant Dr. @NReguart reminds us of the heterogeneity of stage III NSCLC and our teaching has been to determine resectability before treatment. The INCREASE study starts to challenge that. #ESMO22

The difference here is radiation and in T3/T4 NSCLC, local control is so critical. Largely unexplored to date. The INCREASE study explores quad-modality therapy and the results were quite impressive. High pCR rates and seen across PDL1 strata, not just in PDL1 high. #ESMO22




#ESMO22 High G3 TRAE rates but note that use of platinum + etoposide was common and many of these may have been paper toxicities. Any grade pneumonitis only 11% (note radiation dose was usually 50 Gy).

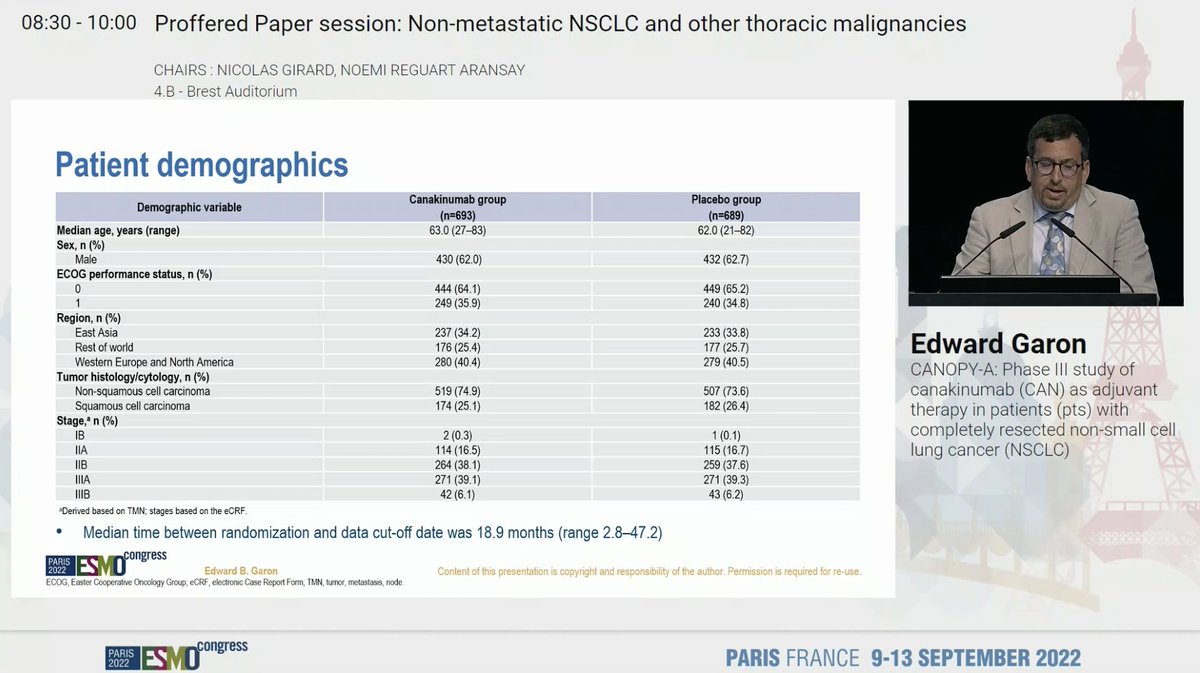
Dr. Eddie Garon presents data from CANOPY-A - adjuvant canakinumab for resected NSCLC #ESMO22

Canakinumab in the CANTOS study was associated with a reduction in NSCLC incidence. Led to CANOPY-A: large study of adjuvant canakinumab after surgery and chemotherapy for NSCLC. #ESMO22


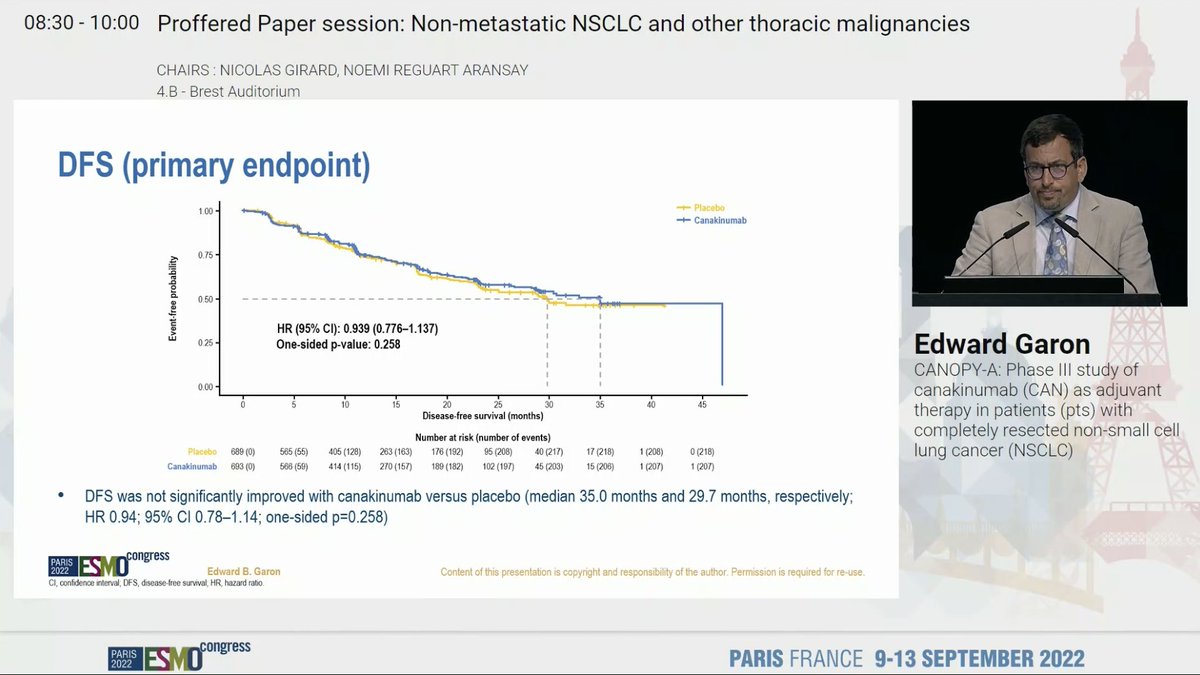
Adjuvant canakinumab did not improve DFS (HR 0.939). CANOPY-A clearly a negative study. #ESMO22
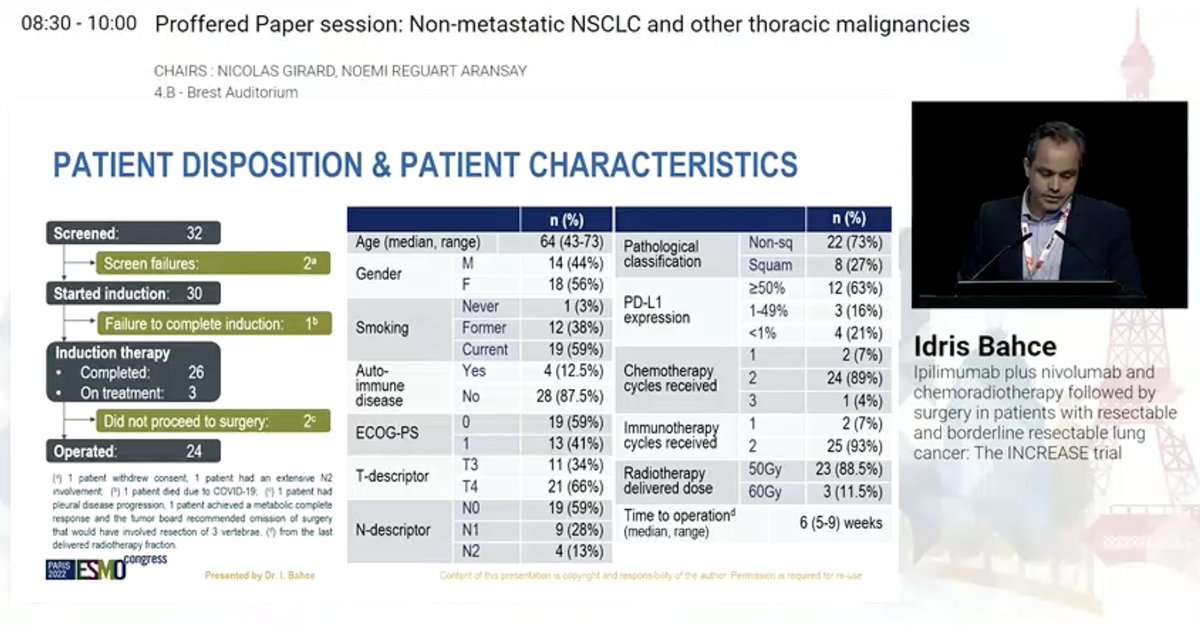
Dr. Idris Bahce presents data from the INCREASE trial - ipilimumab plus nivolumab and chemoradiation followed by surgery in resectable and borderline resectable NSCLC. #ESMO22

Focus is on high T stage and low N stage - not resectable initially but potentially resectable after therapy. Patients here received nivo/ipi on day 1 and nivo on day 22 with chemoradiation then resection 6w later (after restaging) with pCR/MPR primary endpoint. #ESMO22


#ESMO22 Patient disposition here - of 26 patients who completed induction therapy, 3 are still on therapy and 24 completed surgery. Included 66% T4 and 59% N0 (only 13% N2). Majority (63%) had PDL1 high disease. There was one G5 AE (COVID). No AE prevented surgery.


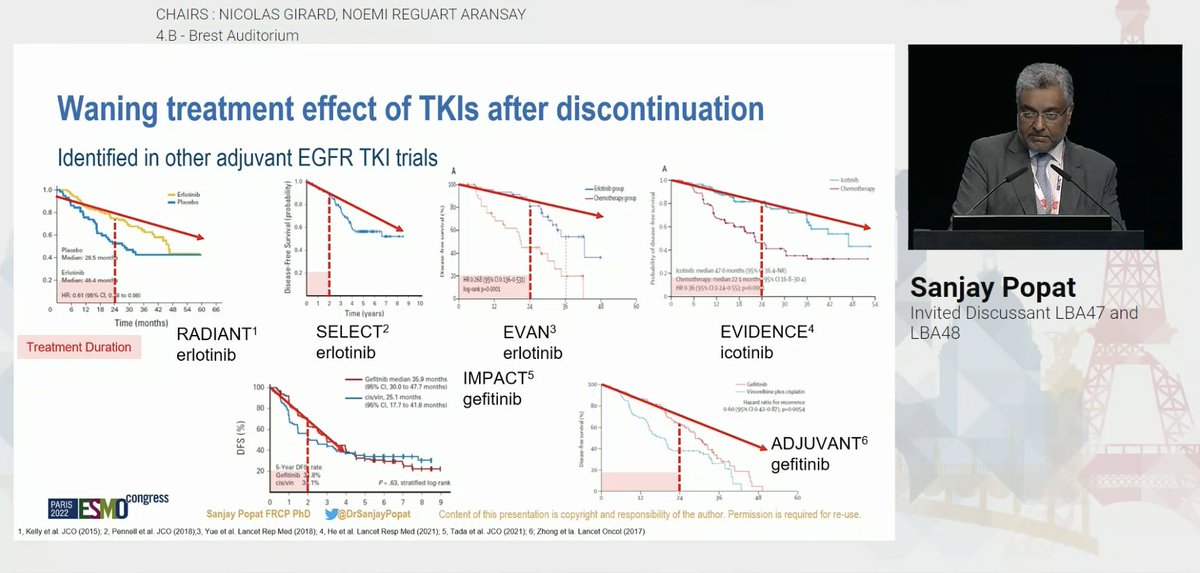
@DrSanjayPopat @myESMO #ESMO22 @DrSanjayPopat points out that the DFS HR is on par with the original analysis but the shape of the curves is different, especially for stage II/III



This is not new - we see a rise in recurrence once TKI is stopped in multiple other adjuvant TKI studies. Is this suggestive of cure or just proper therapy of unidentified (micro)metastatic cancer? #ESMO22
Professor Masahiro Tsuboi presents an important update on ADAURA (adjuvant osimertinib for #EGFR NSCLC) #ESMO22

The DFS HR of 0.23 in resected stage II/III remains very impressive. But once osimertinib is stopped after 3y, the curves do seem to be coming closer together. DFS at 2y with osi is 90% and at 3y is 84% but drops to 70% at 4y. Are we preventing recurrence or delaying it? #ESMO22

#ESMO22 in the overall population, similar trends. Off therapy, DFS curves start to approach. Same trends across stages - though I feel more noticeable in stage III (using AJCC 7 or 8).




#ESMO22 Presidential Symposium 1 LBA3 TIL vs ipilimumab for advanced melanoma, phase 3 study @HaanenJohn @OncoAlert @myESMO
Unresectable stage IIC-IV melanoma progression with a max of 1 line of prior systemic treatment (not ipi), N = 168, randomized 1:1 TIL vs ipilimumab. Primary EP = PFS; Most pts had prior anti PD-1 treatment



PFS significantly improved with TIL vs ipi (Median PFS: 7.2 vs 3.1 mo). HR = 0.50, P < .001. The majority of predefined subgroups benefited from TIL



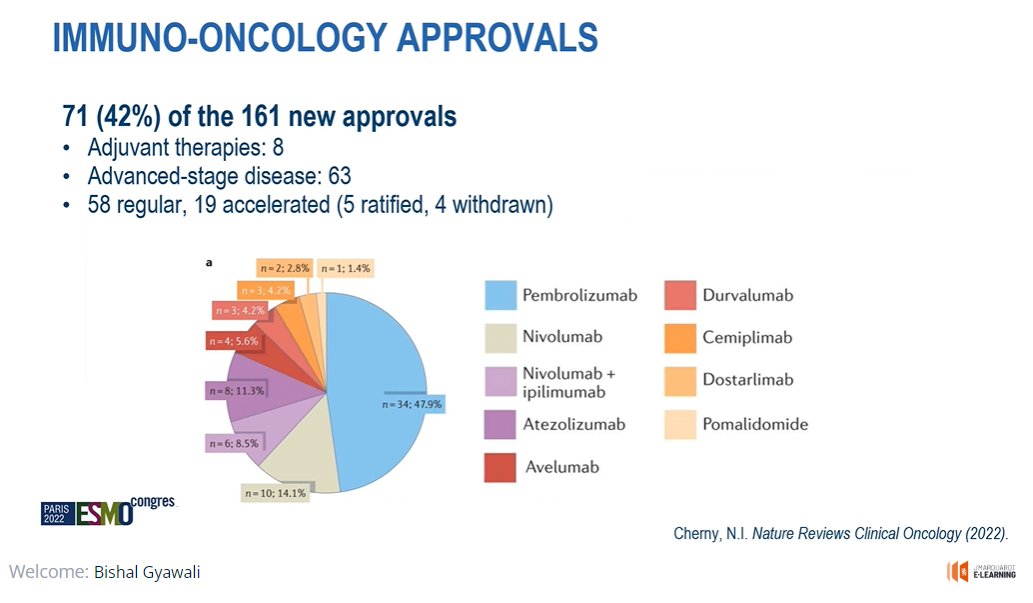
This is going to be a thread of our #MCBS session starting in a couple of minutes at #ESMO22. Follow along for a LIVE tweet-summary of our session! @myESMO @ChernyNathan @VriesElisabeth 1/
First, @ChernyNathan is giving an overview of cancer drugs approved by FDA in last 5 years. For more, read his excellent paper in @NatRevClinOncol published earlier this year. @DianaNrco
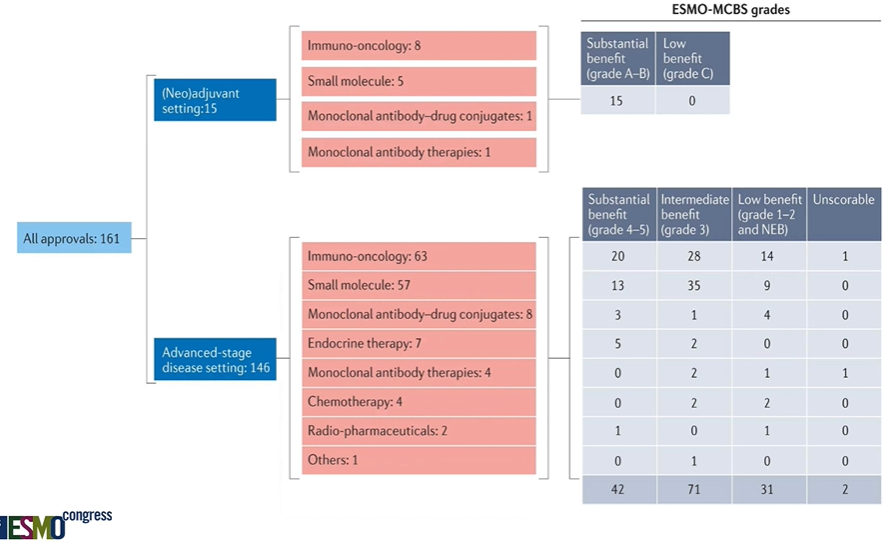
IO drugs made up almost half of these drug approvals. #ESMO22