Discover and read the best of Twitter Threads about #idgrandrounds
Most recents (20)

#idgrandrounds
Presented by @LParraRod
1/2
Man in his 60's, on-going temozolamide + dexa for glioblastoma, p/w 1 wk b/l knee arthritis, preceded by 4 d fever & watery diarrhea.
H/o DLBCL in remission x 4 yrs, mild b/l knee OA
Recently stopped TMP-SMX for unclear reason.
Presented by @LParraRod
1/2
Man in his 60's, on-going temozolamide + dexa for glioblastoma, p/w 1 wk b/l knee arthritis, preceded by 4 d fever & watery diarrhea.
H/o DLBCL in remission x 4 yrs, mild b/l knee OA
Recently stopped TMP-SMX for unclear reason.
2/2
Immigrated to the US from El Salvador 20 yrs ago. No recent travel, pets, illicits. Lives in IL.
WBC 3.6. CMP u/r
Synovial fluid: WBC 85K (80%N)
Approach, DDx? @TxID_Edu @CarlosSaldana @k_vaishnani @VarunPhadke2 @UAB_ID @BIDMC_IDFellows @IUIDfellowship @LeMiguelChavez
Immigrated to the US from El Salvador 20 yrs ago. No recent travel, pets, illicits. Lives in IL.
WBC 3.6. CMP u/r
Synovial fluid: WBC 85K (80%N)
Approach, DDx? @TxID_Edu @CarlosSaldana @k_vaishnani @VarunPhadke2 @UAB_ID @BIDMC_IDFellows @IUIDfellowship @LeMiguelChavez
1/12
CASE RESOLUTION:
Blood & synovial fluid culture +Salmonella typhimurium
Great job! All of you got the right answer and included the most important differential diagnoses.
Takeaway points from this case: approach to arthritis & diarrhea, implications of temazolamide Tx
CASE RESOLUTION:
Blood & synovial fluid culture +Salmonella typhimurium
Great job! All of you got the right answer and included the most important differential diagnoses.
Takeaway points from this case: approach to arthritis & diarrhea, implications of temazolamide Tx
1/3
Sorry guys for the short hiatus. But I’m back! Let’s start with an #idgrandrounds case (as always, patient info modified for privacy)
👉 36/M w/ HIV, p/w GTC seizure. No prodrome. No fever, chills, headache, vision changes
@LeMiguelChavez @NNolanMD @Jncherabie @arauseomd
Sorry guys for the short hiatus. But I’m back! Let’s start with an #idgrandrounds case (as always, patient info modified for privacy)
👉 36/M w/ HIV, p/w GTC seizure. No prodrome. No fever, chills, headache, vision changes
@LeMiguelChavez @NNolanMD @Jncherabie @arauseomd
2/3
2 mos ago, admitted +confusion. That time, CD4 40, VL 4M. Extensive w/u (-): n/l brain MRI, LP (0 WBC, n/l TP/gluc), (-)ID w/u including crypto, JC, EBV, CMV, Toxo. Toxo IgG(-). CT: n/l. ART started
Current admission:
Exam: T 37. Somnolent, no deficits.
Labs: CD4 380, VL 7K
2 mos ago, admitted +confusion. That time, CD4 40, VL 4M. Extensive w/u (-): n/l brain MRI, LP (0 WBC, n/l TP/gluc), (-)ID w/u including crypto, JC, EBV, CMV, Toxo. Toxo IgG(-). CT: n/l. ART started
Current admission:
Exam: T 37. Somnolent, no deficits.
Labs: CD4 380, VL 7K
3/3
Brain MRI: 4 ring-enhancing masses surrounded by edema L frontal lobe. LP: 10 WBC, (-)Toxo, EBV, JC, CMV, VDRL, AFB. Fungal(-). CT: scattered lung nodules.
No prior OI, (-)IGRAs,(-)drug use, (-)exposure/travel
Thoughts? @TxID_Edu @VarunPhadke2 @TMcCarty2010 @BradCutrellMD
Brain MRI: 4 ring-enhancing masses surrounded by edema L frontal lobe. LP: 10 WBC, (-)Toxo, EBV, JC, CMV, VDRL, AFB. Fungal(-). CT: scattered lung nodules.
No prior OI, (-)IGRAs,(-)drug use, (-)exposure/travel
Thoughts? @TxID_Edu @VarunPhadke2 @TMcCarty2010 @BradCutrellMD
#idgrandrounds
1/2
32 F w multiple sclerosis on rituximab, +10d fever, R knee pain in December. Had dysuria tx w/ TMP/SMX 1 wk prior. No trauma. Exam: swollen/tender R knee. No rash. Purulent synovial fluid: 60,000 cells 70%N. Multiple synovial/blood bacteria/fungal/AFB Cx (-)
1/2
32 F w multiple sclerosis on rituximab, +10d fever, R knee pain in December. Had dysuria tx w/ TMP/SMX 1 wk prior. No trauma. Exam: swollen/tender R knee. No rash. Purulent synovial fluid: 60,000 cells 70%N. Multiple synovial/blood bacteria/fungal/AFB Cx (-)
2/2
No response w/ cefe/vanc. GC/CT(-), HIV(-), Q/Brucella(-), fungal studies(-).
Lives in rural IL, no travel. Denies substance use. Single, sexually active w/ 1 partner. No pets. Unemployed.
Thoughts & DDX? @VarunPhadke2 @TxID_Edu @k_vaishnani @Cortes_Penfield @jdcooperid
No response w/ cefe/vanc. GC/CT(-), HIV(-), Q/Brucella(-), fungal studies(-).
Lives in rural IL, no travel. Denies substance use. Single, sexually active w/ 1 partner. No pets. Unemployed.
Thoughts & DDX? @VarunPhadke2 @TxID_Edu @k_vaishnani @Cortes_Penfield @jdcooperid
1/12
Case resolution:
▪️Synovial fluid PCR +Mycoplasma/Ureaplasma
▪️Successfully tx w/ doxy
Diagnosis: Mycoplasma/Ureaplasma septic arthritis
Good job all of you! @TxID_Edu @VarunPhadke2 @CrystalZhengMD @RashDecisionz @vjhaveri27 @KartikAcharyaID @k_vaishnani
Case resolution:
▪️Synovial fluid PCR +Mycoplasma/Ureaplasma
▪️Successfully tx w/ doxy
Diagnosis: Mycoplasma/Ureaplasma septic arthritis
Good job all of you! @TxID_Edu @VarunPhadke2 @CrystalZhengMD @RashDecisionz @vjhaveri27 @KartikAcharyaID @k_vaishnani
#idgrandrounds
1/2
68/M +progressive L facial/arm numbness & weakness, R hip pain x 6 wks. +malaise/wt loss but no fever. Exam: no rashes, +dysarthria. Labs: U/R.
Brain MRI: 2x2 cm R thalamic mass w/ vaso edema
CT: speculated RUL mass, sclerotic R iliac crest/SI joint
👇
1/2
68/M +progressive L facial/arm numbness & weakness, R hip pain x 6 wks. +malaise/wt loss but no fever. Exam: no rashes, +dysarthria. Labs: U/R.
Brain MRI: 2x2 cm R thalamic mass w/ vaso edema
CT: speculated RUL mass, sclerotic R iliac crest/SI joint
👇
2/2
Lives in rural IL near a creek. Stays at home w/ a dog. Loves to garden. No travel, incarceration.
Neurosurgery performed burr hole/biopsy of mass (c/f glioblastoma). ID was consulted when biopsy came out.
What is your ddx/dx? @TxID_Edu @jdcooperid @GermHunterMD
Lives in rural IL near a creek. Stays at home w/ a dog. Loves to garden. No travel, incarceration.
Neurosurgery performed burr hole/biopsy of mass (c/f glioblastoma). ID was consulted when biopsy came out.
What is your ddx/dx? @TxID_Edu @jdcooperid @GermHunterMD
1/11 Biopsy of brain mass: broad-based budding yeast, Cx: Blastomyces dermatitidis. Urine Histo Ag: low positive
CASE RESOLUTION: Disseminated blastomycosis
@LemuelNonMD @TxID_Edu @Cortes_Penfield @KartikAcharyaID @IDdoc_Vetri @jdcooperid got the correct Dx/Ddx! Thank you.
CASE RESOLUTION: Disseminated blastomycosis
@LemuelNonMD @TxID_Edu @Cortes_Penfield @KartikAcharyaID @IDdoc_Vetri @jdcooperid got the correct Dx/Ddx! Thank you.
#idgrandrounds
48F, bitten by a monkey at a zoo. She calls her primary who then calls you for advice.
What Qs should you ask? What infections should you be worried about? @TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid
Have you had a consult on monkey bite before?
48F, bitten by a monkey at a zoo. She calls her primary who then calls you for advice.
What Qs should you ask? What infections should you be worried about? @TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid
Have you had a consult on monkey bite before?
@TxID_Edu @Cortes_Penfield @BradCutrellMD @jdcooperid 1/15
Great! Thank you for ALL your responses. Speical thanks to @TxID_Edu @vivax74 @VarunPhadke2 @10minus6cosm for referencing additional resources.
Hope this tweetorial helps, especially those who may get consulted on monkey bite/exposure in the future.
Follow the thread 👇
Great! Thank you for ALL your responses. Speical thanks to @TxID_Edu @vivax74 @VarunPhadke2 @10minus6cosm for referencing additional resources.
Hope this tweetorial helps, especially those who may get consulted on monkey bite/exposure in the future.
Follow the thread 👇
2/15
𝐖𝐡𝐚𝐭 𝐢𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐧𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐲𝐨𝐮 𝐛𝐞 𝐰𝐨𝐫𝐫𝐢𝐞𝐝 𝐚𝐛𝐨𝐮𝐭?
A LOT, but the most important ones are:
1⃣ Herpes B
2⃣ Rabies
3⃣ Tetanus
Let's talk a little bit more about Herpes B and rabies 👇
𝐖𝐡𝐚𝐭 𝐢𝐧𝐟𝐞𝐜𝐭𝐢𝐨𝐧𝐬 𝐬𝐡𝐨𝐮𝐥𝐝 𝐲𝐨𝐮 𝐛𝐞 𝐰𝐨𝐫𝐫𝐢𝐞𝐝 𝐚𝐛𝐨𝐮𝐭?
A LOT, but the most important ones are:
1⃣ Herpes B
2⃣ Rabies
3⃣ Tetanus
Let's talk a little bit more about Herpes B and rabies 👇
#idgrandrounds
(Part 1 of 2)
31M carpenter from the Midwest, +3 wks b/l blurred vision/eye redness. No pain/discharge, floaters, (+)photophobia/hearing impairment. No headache, fever, N/V. Found to have new HIV dx (CD4 520 VL 120K). Exam: b/l red eyes, nonfocal neuro, no rash.
(Part 1 of 2)
31M carpenter from the Midwest, +3 wks b/l blurred vision/eye redness. No pain/discharge, floaters, (+)photophobia/hearing impairment. No headache, fever, N/V. Found to have new HIV dx (CD4 520 VL 120K). Exam: b/l red eyes, nonfocal neuro, no rash.
#idgrandrounds
(Part 2 of 2)
(-)RPR/TSPOT. N/l CBC/CMP. Optho: +uveitis.
(-)PMH/illicits. MSM. No h/o travel/pets. Brief h/o homelessness but no h/o incarceration.
Differential dx? @CPSolvers @TxID_Edu @jdcooperid @BradCutrellMD @Cortes_Penfield @MohitHarshMD @serotavirus
(Part 2 of 2)
(-)RPR/TSPOT. N/l CBC/CMP. Optho: +uveitis.
(-)PMH/illicits. MSM. No h/o travel/pets. Brief h/o homelessness but no h/o incarceration.
Differential dx? @CPSolvers @TxID_Edu @jdcooperid @BradCutrellMD @Cortes_Penfield @MohitHarshMD @serotavirus
@CPSolvers @TxID_Edu @jdcooperid @BradCutrellMD @Cortes_Penfield @MohitHarshMD @serotavirus #idgrandrounds
1/11
𝐏𝐑𝐎𝐙𝐎𝐍𝐄 was suspected. Diluted sample showed RPR to be 1:1024.
LP was performed and showed evidence of lymphocytic pleocytosis and with a +VDRL.
CASE RESOLUTION: Neuro-ocular syphilis, w/ prozone reaction
1/11
𝐏𝐑𝐎𝐙𝐎𝐍𝐄 was suspected. Diluted sample showed RPR to be 1:1024.
LP was performed and showed evidence of lymphocytic pleocytosis and with a +VDRL.
CASE RESOLUTION: Neuro-ocular syphilis, w/ prozone reaction
#idgrandrounds
1/2
61M ESRD s/p kidney transplant 2016 (CMV D-/R-), on tac/pred, 6 mos progressive memory loss, falls, headache, blurred vision. No fever.
Traveled to southwest US, Malaysia, Thailand >10 yrs ago. Monogamous relationship.
@BradCutrellMD @Cortes_Penfield
1/2
61M ESRD s/p kidney transplant 2016 (CMV D-/R-), on tac/pred, 6 mos progressive memory loss, falls, headache, blurred vision. No fever.
Traveled to southwest US, Malaysia, Thailand >10 yrs ago. Monogamous relationship.
@BradCutrellMD @Cortes_Penfield
2/2
Exam: disoriented, poor memory, ⬇️ proprioreception, supple neck.
Labs: macrocytic anemia
CXR: nonspecific small nodule
MRI: mild periventricular hyperintensity, panventriculomegaly
What are you DDX and suggested work-up? @TxID_Edu @jdcooperid @MohitHarshMD @k_vaishnani
Exam: disoriented, poor memory, ⬇️ proprioreception, supple neck.
Labs: macrocytic anemia
CXR: nonspecific small nodule
MRI: mild periventricular hyperintensity, panventriculomegaly
What are you DDX and suggested work-up? @TxID_Edu @jdcooperid @MohitHarshMD @k_vaishnani
@TxID_Edu @jdcooperid @MohitHarshMD @k_vaishnani 1/11
CASE RESOLUTION
Prior to transfer, managed in the dementia clinic.
LP was only done late: lymphocytic pleocytosis, elevated TP, glucose <20. Serum/CSF CrAg +, CSF +Cryptococcus neoformans.
Excellent work @Cortes_Penfield @jdcooperid @TxID_Edu @ShohamTxID @PVishnuRao1
CASE RESOLUTION
Prior to transfer, managed in the dementia clinic.
LP was only done late: lymphocytic pleocytosis, elevated TP, glucose <20. Serum/CSF CrAg +, CSF +Cryptococcus neoformans.
Excellent work @Cortes_Penfield @jdcooperid @TxID_Edu @ShohamTxID @PVishnuRao1
#idgrandrounds
32F w/ HIV, stared ART 9 mos ago (CD4 90, now 170), p/w 4 wks, slightly tender, hypertrophic vulvar lesion (representative pic 👇). Lives in US. Biopsy: no malignancy, culture (-).
Diagnosis? Differentials? @TxID_Edu @BradCutrellMD @DocWoc71 @Cortes_Penfield
32F w/ HIV, stared ART 9 mos ago (CD4 90, now 170), p/w 4 wks, slightly tender, hypertrophic vulvar lesion (representative pic 👇). Lives in US. Biopsy: no malignancy, culture (-).
Diagnosis? Differentials? @TxID_Edu @BradCutrellMD @DocWoc71 @Cortes_Penfield

@TxID_Edu @BradCutrellMD @DocWoc71 @Cortes_Penfield 1/9
PCR, histopath c/w HSV. Failed to respond to valacyclovir, foscarnet (viral culture w/ no resistance). Cured w/ surgical resection + valacyclovir.
CASE RESOLUTION: 𝐇𝐞𝐫𝐩𝐞𝐬 𝐯𝐞𝐠𝐞𝐭𝐚𝐧𝐬 (hypertrophic HSV)
Picture in MCQ from: researchgate.net/publication/23…
PCR, histopath c/w HSV. Failed to respond to valacyclovir, foscarnet (viral culture w/ no resistance). Cured w/ surgical resection + valacyclovir.
CASE RESOLUTION: 𝐇𝐞𝐫𝐩𝐞𝐬 𝐯𝐞𝐠𝐞𝐭𝐚𝐧𝐬 (hypertrophic HSV)
Picture in MCQ from: researchgate.net/publication/23…

2/9
Typical illness script for HSV esp in immunocompetent patients:
✔️ painful ulcers, vesicles/group of vesicles that ulcerate
Among immunocompromised patients, HSV can also manifest atypically. 𝐇𝐞𝐫𝐩𝐞𝐬 𝐯𝐞𝐠𝐞𝐭𝐚𝐧𝐬 is one of the atypical HSV manifestations.
Typical illness script for HSV esp in immunocompetent patients:
✔️ painful ulcers, vesicles/group of vesicles that ulcerate
Among immunocompromised patients, HSV can also manifest atypically. 𝐇𝐞𝐫𝐩𝐞𝐬 𝐯𝐞𝐠𝐞𝐭𝐚𝐧𝐬 is one of the atypical HSV manifestations.
Part 1 of 2 | MCQ in 2nd Part 2:
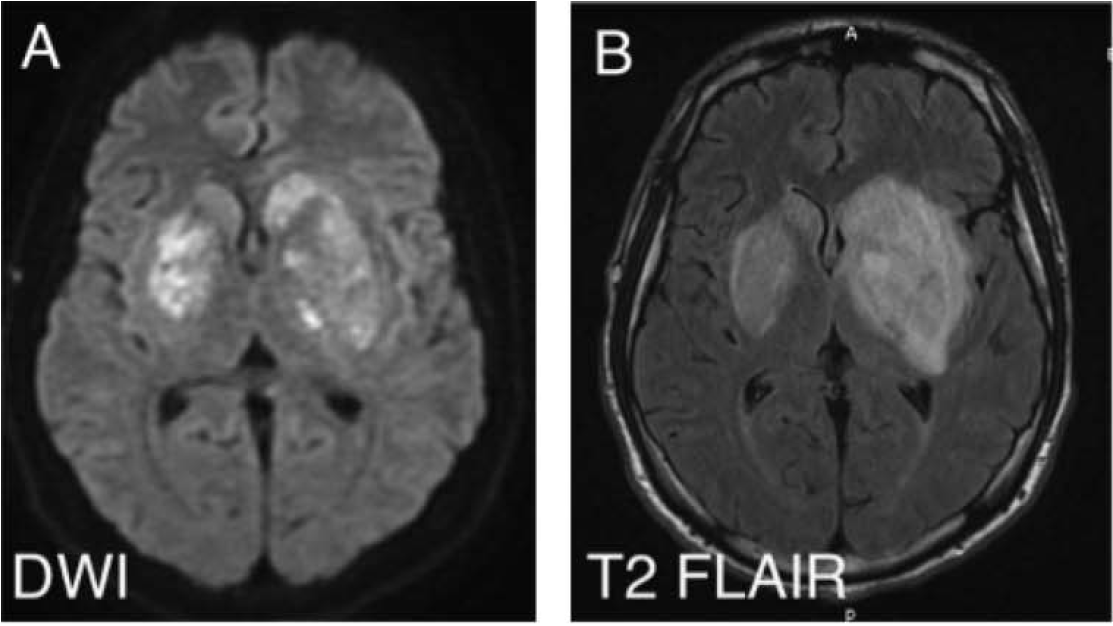
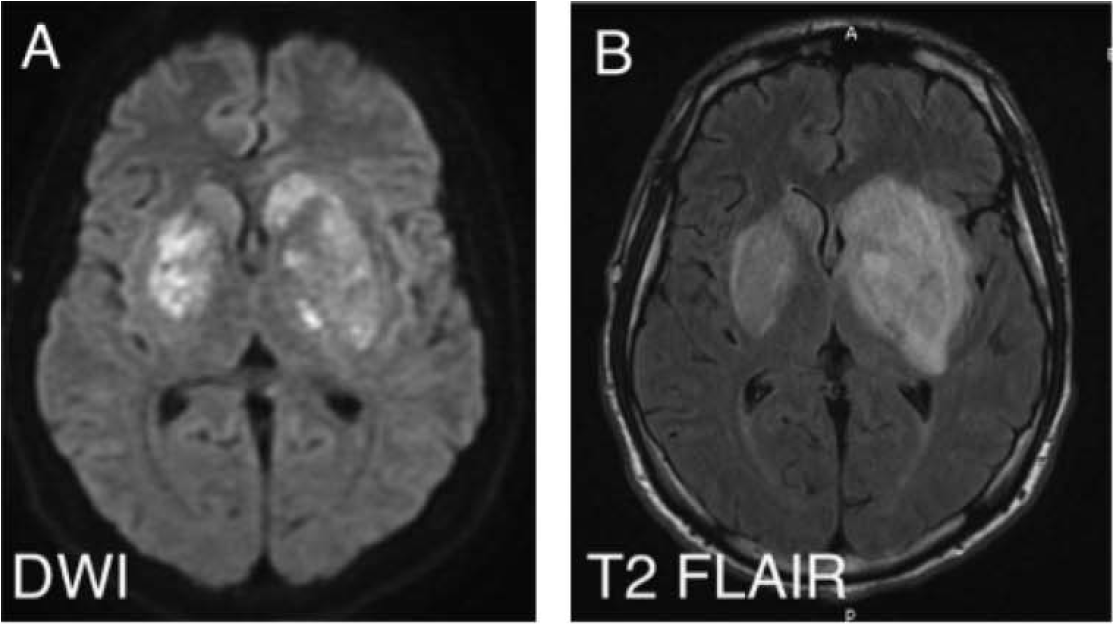
23M active IV heroin user p/w 4 d fever/headache/seizure. Temp 39.3, supple neck. Initial head CT (-). CSF: WBC 30 (60% L), TP 90, gluc n/l. Developed R arm/leg hemiparesis hospital day 5. MRI: large L>R b/l basal ganglia enhancing lesions (👇)
23M active IV heroin user p/w 4 d fever/headache/seizure. Temp 39.3, supple neck. Initial head CT (-). CSF: WBC 30 (60% L), TP 90, gluc n/l. Developed R arm/leg hemiparesis hospital day 5. MRI: large L>R b/l basal ganglia enhancing lesions (👇)
|Part 2 of 2 |
Routine CSF viral PCRs/bacterial/AFB/fungal Cxs (-). Blood Cxs, HIV, RPR, TEE (-). Lives in Missouri, no travel/other exposures. Continued to be highly febrile on cefepime/vancomycin/metronidazole. What is the most likely cause of his clinical presentation?
Routine CSF viral PCRs/bacterial/AFB/fungal Cxs (-). Blood Cxs, HIV, RPR, TEE (-). Lives in Missouri, no travel/other exposures. Continued to be highly febrile on cefepime/vancomycin/metronidazole. What is the most likely cause of his clinical presentation?
1/9
Only 37% got the correct answer, Mucor.
Learning points:
✔️ High risk of cerebral mucormycosis among people who inject drugs (PWID)
✔️ Unique basal ganglia involvement seen in these cases
Picture in MCQ taken from:
ncbi.nlm.nih.gov/pmc/articles/P…
Only 37% got the correct answer, Mucor.
Learning points:
✔️ High risk of cerebral mucormycosis among people who inject drugs (PWID)
✔️ Unique basal ganglia involvement seen in these cases
Picture in MCQ taken from:
ncbi.nlm.nih.gov/pmc/articles/P…
#IDgrandrounds
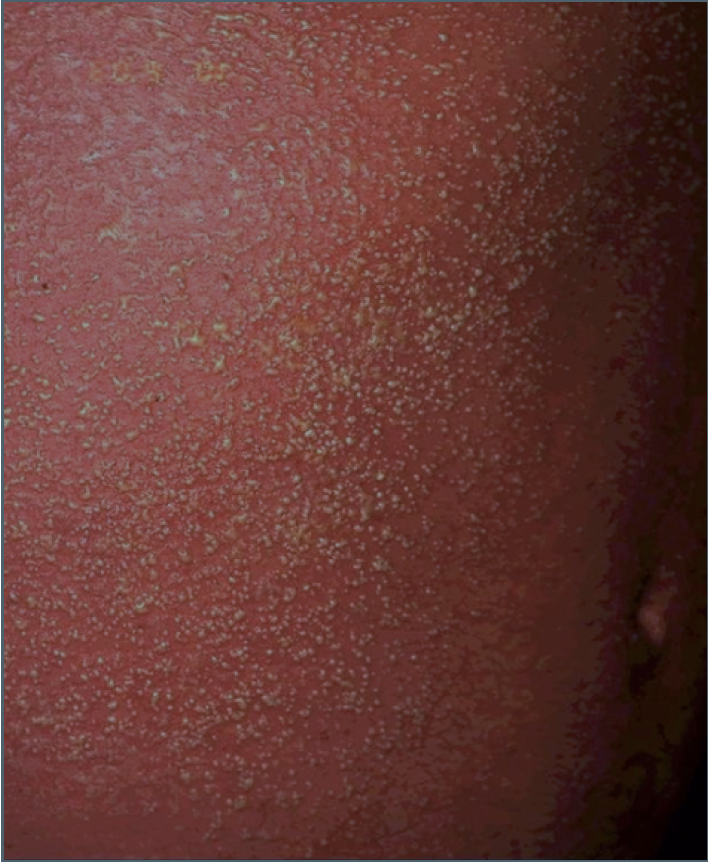
35F, from St. Louis, woke up w/ a mildly painful bruise L arm, the next day, +diffuse erythematous rash, fever, abdominal pain. Unremarkable VS/labs. Representative pics of rashes 👇.
Diagnosis? Differentials? @TxID_Edu @BradCutrellMD @Cortes_Penfield @DocWoc71
35F, from St. Louis, woke up w/ a mildly painful bruise L arm, the next day, +diffuse erythematous rash, fever, abdominal pain. Unremarkable VS/labs. Representative pics of rashes 👇.
Diagnosis? Differentials? @TxID_Edu @BradCutrellMD @Cortes_Penfield @DocWoc71

@TxID_Edu @BradCutrellMD @Cortes_Penfield @DocWoc71 1/9
Case continued:
Bruise evolved into an ulcer. On further questioning, reported seeing spider close to her bed prior
CASE RESOLUTION:
Acute generalized exanthematous pustulosis (AGEP) 2/2 spider bite
Pics in MCQ:
medicaljournals.se/acta/content/h…
flickr.com/photos/1448153…
Case continued:
Bruise evolved into an ulcer. On further questioning, reported seeing spider close to her bed prior
CASE RESOLUTION:
Acute generalized exanthematous pustulosis (AGEP) 2/2 spider bite
Pics in MCQ:
medicaljournals.se/acta/content/h…
flickr.com/photos/1448153…
2/9
The rash a/w AGEP is characteristic:
▪️ Diffuse erythema
▪️ Innumerable, pinhead-sized pustules
@TxID_Edu @rloganjonesmd @PVishnuRao1 @alxpenguin @npowah @dschless immediately suspected AGEP! Nice job!
The rash a/w AGEP is characteristic:
▪️ Diffuse erythema
▪️ Innumerable, pinhead-sized pustules
@TxID_Edu @rloganjonesmd @PVishnuRao1 @alxpenguin @npowah @dschless immediately suspected AGEP! Nice job!
#IDgrandrounds
30M +fever, ab pain, cough x 1wk. Back from Tanzania (swam in Lake Victoria) 2 mos ago. +vaccination/malaria prophy before trip. Blood smears (-). Eosinophil count 4,000.
Diagnosis/differentials? @Cortes_Penfield @TxID_Edu @BradCutrellMD @DocWoc71 @Darcy_ID_doc
30M +fever, ab pain, cough x 1wk. Back from Tanzania (swam in Lake Victoria) 2 mos ago. +vaccination/malaria prophy before trip. Blood smears (-). Eosinophil count 4,000.
Diagnosis/differentials? @Cortes_Penfield @TxID_Edu @BradCutrellMD @DocWoc71 @Darcy_ID_doc


@Cortes_Penfield @TxID_Edu @BradCutrellMD @DocWoc71 @Darcy_ID_doc 1/10
Thank you for all your responses! @TxID_Edu @BradCutrellMD @DocWoc71 @GermHunterMD @marschall_jonas @jdcooperid others
Stool sample demonstrated Schistosoma mansoni eggs.
CASE RESOLUTION: Acute schistosomiasis (Katayama fever)
mcdinternational.org/trainings/mala…
Thank you for all your responses! @TxID_Edu @BradCutrellMD @DocWoc71 @GermHunterMD @marschall_jonas @jdcooperid others
Stool sample demonstrated Schistosoma mansoni eggs.
CASE RESOLUTION: Acute schistosomiasis (Katayama fever)
mcdinternational.org/trainings/mala…

2/10
Katayama fever was previously covered here last year. Click below to review:
What I'd like to talk about briefly is my "𝔸𝔹ℂ𝔻𝔼" approach to generating an illness script for a febrile returned traveler.
Katayama fever was previously covered here last year. Click below to review:
What I'd like to talk about briefly is my "𝔸𝔹ℂ𝔻𝔼" approach to generating an illness script for a febrile returned traveler.
#IDgrandrounds
40M, late summer, +sudden R facial weakness, diplopia, dysphagia; later,+UE weakness; lives in Colorado, loves to hike, had a lot of tick bites.
What are your differential Dx?
@BradCutrellMD @Cortes_Penfield @DocWoc71 @Darcy_ID_doc @TxID_Edu @GermHunterMD
40M, late summer, +sudden R facial weakness, diplopia, dysphagia; later,+UE weakness; lives in Colorado, loves to hike, had a lot of tick bites.
What are your differential Dx?
@BradCutrellMD @Cortes_Penfield @DocWoc71 @Darcy_ID_doc @TxID_Edu @GermHunterMD
@BradCutrellMD @Cortes_Penfield @DocWoc71 @Darcy_ID_doc @TxID_Edu @GermHunterMD 1/10
CASE CONTINUED.
Stroke team activated upon ED arrival.
2 household members were rushed to the hospital for paralysis & respiratory compromise. Unfortunately, both died. All reported consuming home-canned food.
ID was called. CDC alerted & antitoxin flown in.
CASE CONTINUED.
Stroke team activated upon ED arrival.
2 household members were rushed to the hospital for paralysis & respiratory compromise. Unfortunately, both died. All reported consuming home-canned food.
ID was called. CDC alerted & antitoxin flown in.

2/10
CASE RESOLUTION: Foodborne botulism
@Cortes_Penfield @TxID_Edu @BradCutrellMD & @JIOReilly highlighted the important DDx for this case.
Many ID Dx can p/w various neuro ssx depending on the direct/indirect involvement of the central/peripheral nervous system
CASE RESOLUTION: Foodborne botulism
@Cortes_Penfield @TxID_Edu @BradCutrellMD & @JIOReilly highlighted the important DDx for this case.
Many ID Dx can p/w various neuro ssx depending on the direct/indirect involvement of the central/peripheral nervous system
#IDgrandrounds #3
1/4
51/M, receiving vancomycin & cefepime for osteomyelitis, developed diffuse bullous lesions (trunk, extremities, buttocks)
Dx: vancomycin-induced linear IgA bullous dermatosis (LABD)
1/4
51/M, receiving vancomycin & cefepime for osteomyelitis, developed diffuse bullous lesions (trunk, extremities, buttocks)
Dx: vancomycin-induced linear IgA bullous dermatosis (LABD)
2/4
Vancomyin-induced LABD
-- most common drug a/w LABD (others: lithium, phenytoin, TMP/SMX, furosemide, atorvastatin, dicolfenac)
-- severity NOT correlated w/ serum vanc level
-- onset: 2-21 days after start
-- Tx: D/c vancomycin --> time to resolution 2 d to 4 wks
Vancomyin-induced LABD
-- most common drug a/w LABD (others: lithium, phenytoin, TMP/SMX, furosemide, atorvastatin, dicolfenac)
-- severity NOT correlated w/ serum vanc level
-- onset: 2-21 days after start
-- Tx: D/c vancomycin --> time to resolution 2 d to 4 wks
3/4
Vancomycin-induced LABD
-- characterized by Ig A deposition in the dermoepidermal junction --> bullae is TENSE
-- tense bullae distinguishes it from drug-induced SJS/TEN (intraepidermal pathology ▶️ flaccid bullae ▶️ +Nikolsky's sign)
Vancomycin-induced LABD
-- characterized by Ig A deposition in the dermoepidermal junction --> bullae is TENSE
-- tense bullae distinguishes it from drug-induced SJS/TEN (intraepidermal pathology ▶️ flaccid bullae ▶️ +Nikolsky's sign)
#IDgrandrounds #2
1/6
4-day old infant presents from home w/ fever and seizure. Brain MRI: diffuse diffusion restriction. All w/u (-) except multiplex PCR: influenza A!
Dx: neonatal influenza A, acute encephalopathy w/ biphasic seizures and late reduced diffusion (AESD)
1/6
4-day old infant presents from home w/ fever and seizure. Brain MRI: diffuse diffusion restriction. All w/u (-) except multiplex PCR: influenza A!
Dx: neonatal influenza A, acute encephalopathy w/ biphasic seizures and late reduced diffusion (AESD)
2/6
Neonatal influenza
-- trans placental possible but most commonly POSTNATAL acquisition
-- more SEVERE disease than older children & adults
-- prevention: IMMUNIZATION of caregivers/family, immunization of pregnant women
#WhyIVaccinate @IDSAInfo #IDWeek2019
Neonatal influenza
-- trans placental possible but most commonly POSTNATAL acquisition
-- more SEVERE disease than older children & adults
-- prevention: IMMUNIZATION of caregivers/family, immunization of pregnant women
#WhyIVaccinate @IDSAInfo #IDWeek2019
3/6
Influenza-associated neurological disease
-- 1st reported in 1918
-- most cases in children
-- pleocytosis is often absent
-- spectrum of disease (see pic👇)
ncbi.nlm.nih.gov/pubmed/24352349
Influenza-associated neurological disease
-- 1st reported in 1918
-- most cases in children
-- pleocytosis is often absent
-- spectrum of disease (see pic👇)
ncbi.nlm.nih.gov/pubmed/24352349

1/5
#IDgrandrounds
Teenager, h/o vaping, admitted w/ prolonged fever, cough, SOB, respiratory failure. CXR/CT: diffuse infiltrates. No response to antibiotics. Multiple ID/Rheum w/u (-). BAL +lipid-laden macrophages.
Dx: attributed to vaping-induced lung injury
#IDgrandrounds
Teenager, h/o vaping, admitted w/ prolonged fever, cough, SOB, respiratory failure. CXR/CT: diffuse infiltrates. No response to antibiotics. Multiple ID/Rheum w/u (-). BAL +lipid-laden macrophages.
Dx: attributed to vaping-induced lung injury
2/5
E-cigs (vaping) contain less toxic chemicals than conventional cigs but not harmless. Can contain heavy metals, volatile organic compounds. Been used to deliver not only nicotine but also THC, CBC, butane hash oils.
E-cigs (vaping) contain less toxic chemicals than conventional cigs but not harmless. Can contain heavy metals, volatile organic compounds. Been used to deliver not only nicotine but also THC, CBC, butane hash oils.
3/5
Vaping-induced lung injury
-- Median age 19 (16-53)
-- CAP-like presentation (>80% fever, cough, SOB, WBC >11 w/ PMN)
-- 81% GI ssx (n/v, diarrhea, abdominal pain)
-- 94% hospitalized, 87% received O2, 32% intubation
CXR/CT image:
nejm.org/doi/full/10.10…
Vaping-induced lung injury
-- Median age 19 (16-53)
-- CAP-like presentation (>80% fever, cough, SOB, WBC >11 w/ PMN)
-- 81% GI ssx (n/v, diarrhea, abdominal pain)
-- 94% hospitalized, 87% received O2, 32% intubation
CXR/CT image:
nejm.org/doi/full/10.10…

#IDgrandrounds
1/4)
Case #1: 40s, male, p/w invasive sino-orbital aspergillosis; otherwise healthy, uses inhaled steroids
Case #2: 70s, male, s/p lung TX 7 yrs ago, on pred/tacro/mycophenolate, p/w cryptococcal laryngitis; uses inhaled steroids
1/4)
Case #1: 40s, male, p/w invasive sino-orbital aspergillosis; otherwise healthy, uses inhaled steroids
Case #2: 70s, male, s/p lung TX 7 yrs ago, on pred/tacro/mycophenolate, p/w cryptococcal laryngitis; uses inhaled steroids
2/4) Cases highlight invasive fungal infection risk with inhaled steroid. Remains a rare disease.
CRYPTO LARYNGITIS
-- in one case series: only 28% were immunocompromised, 67% of immunocompetent hosts using inhaled steroids
Case series/picture from:
ncbi.nlm.nih.gov/pubmed/30678486
CRYPTO LARYNGITIS
-- in one case series: only 28% were immunocompromised, 67% of immunocompetent hosts using inhaled steroids
Case series/picture from:
ncbi.nlm.nih.gov/pubmed/30678486

3/4)
CRYPTO LARYNGITIS continued
-- in the case series, only 39% had +CrAg (method used not mentioned)
-- mainstay in diagnosis: biopsy, histopathology, fungal staining
Histopath pics from:
ncbi.nlm.nih.gov/pubmed/30678486
CRYPTO LARYNGITIS continued
-- in the case series, only 39% had +CrAg (method used not mentioned)
-- mainstay in diagnosis: biopsy, histopathology, fungal staining
Histopath pics from:
ncbi.nlm.nih.gov/pubmed/30678486

#IDgrandrounds 30/F, HIV (CD4 25), diffuse (>90% BSA), thick, hyperkeratotic/pigmented plaques w/ extensive flaking x 3 months. No fever/meds.
Peeling similar to this (see picture).
Differentials? @DocWoc71 @CarlosdelRio7 @Cortes_Penfield @SAIRABT @GermHunterMD @CPSolvers
Peeling similar to this (see picture).
Differentials? @DocWoc71 @CarlosdelRio7 @Cortes_Penfield @SAIRABT @GermHunterMD @CPSolvers

@DocWoc71 @CarlosdelRio7 @Cortes_Penfield @SAIRABT @GermHunterMD @CPSolvers 1/10) #IDgrandrounds Case resolution:
Clinical/path dx: erythrodermic psoriasis @dschless @PACinTX
Patient's rash, most impressive I've ever seen. Dramatic improvement w/ infliximab.
Many thanks to our fellow @NNolanMD who did a fantastic presentation last week. @CPSolvers
Clinical/path dx: erythrodermic psoriasis @dschless @PACinTX
Patient's rash, most impressive I've ever seen. Dramatic improvement w/ infliximab.
Many thanks to our fellow @NNolanMD who did a fantastic presentation last week. @CPSolvers
2/10) % of psoriasis in people w/ and w/o HIV are similar. But people with HIV develop more severe & atypical forms of psoriasis (erythroderma, guttate, palmoplantar, +arthritis)
Psoriasis can be a presenting symptom of HIV as reported by @doktora_ging
ncbi.nlm.nih.gov/pmc/articles/P…
Psoriasis can be a presenting symptom of HIV as reported by @doktora_ging
ncbi.nlm.nih.gov/pmc/articles/P…
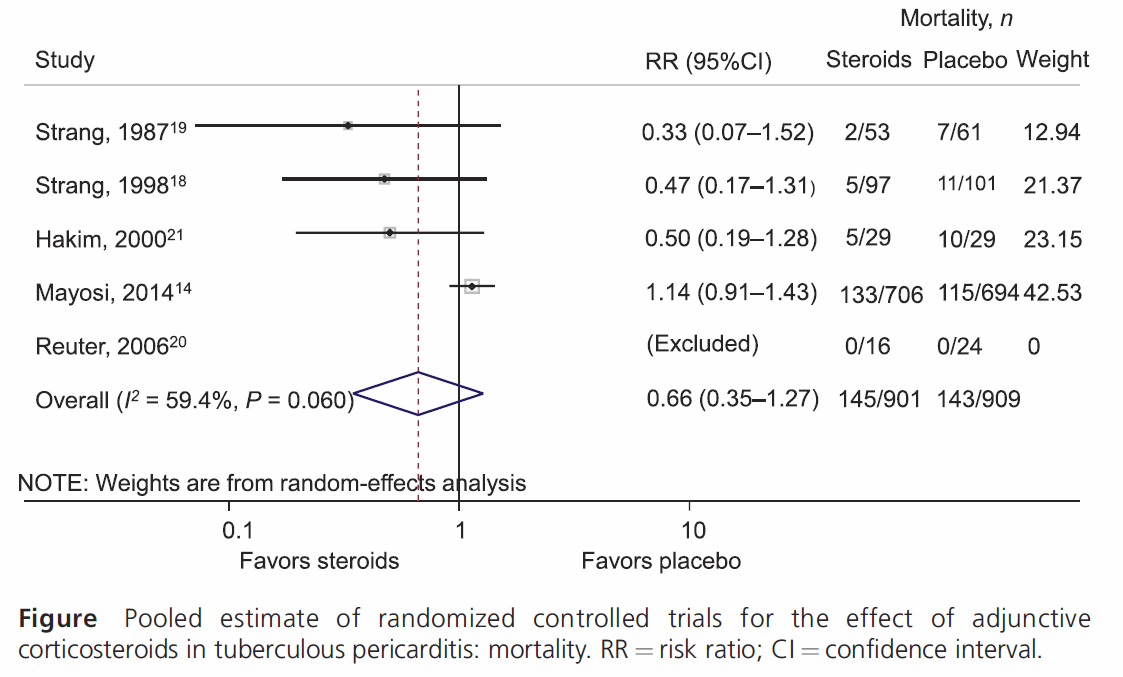
#IDgrandrounds 50/M with new HIV diagnosis (CD4 13), presents with miliary TB and pericarditis (moderate pericardial effusion, no evidence of constrictive physiology). Together with anti-TB medications, will you prescribe corticosteroids?
1/5) No strong evidence to support the use of steroids especially in people w/ HIV.
Guidelines differ however:
ATS/CDC/IDSA 2016 idsociety.org/practice-guide…:
-- initial steroids "not be routinely used"
WHO 2017 who.int/tb/publication…:
-- initial steroids "maybe used"
Guidelines differ however:
ATS/CDC/IDSA 2016 idsociety.org/practice-guide…:
-- initial steroids "not be routinely used"
WHO 2017 who.int/tb/publication…:
-- initial steroids "maybe used"
2/5) A recent meta-analysis (from our very own Dr. Ige George), showed no mortality difference w/ the use of steroids (Forest plot provided in the pic)
ingentaconnect.com/content/iuatld…
ingentaconnect.com/content/iuatld…
#IDgrandrounds 24/F w/ recurrent R arm lymphocutaneous cellulitis after a cat scratch (cat later died). W/u all (-). 16s+ Mycoplasma sp. Case: human hemotropic Mycoplamsa infection, very rare zoonotic infection from cats. ncbi.nlm.nih.gov/pubmed/19046522; wwwnc.cdc.gov/eid/article/14… #IDMedEd
#IDgrandrounds #application Other causes of lymphocutaneous cellulitis (rash + regional lymphadenopathy) #IDMedEd
Staph/Strep
Sporothrix
Bartonella (cat scratch)
Nocardia
Tularemia (ulceroglandular)
Non-TB Mycobacterium
Rat bite fever
Erysipelothrix
Plague
Staph/Strep
Sporothrix
Bartonella (cat scratch)
Nocardia
Tularemia (ulceroglandular)
Non-TB Mycobacterium
Rat bite fever
Erysipelothrix
Plague
#IDgrandrounds #application Classically a/w cat exposure:
("My cat loves PPeanut BBuTTTer") #IDMedEd
Plague
Pasteurella
Bartonella
Bordetella bronchiseptica
Tularemia
Toxoplasma
Toxocara cati
Ultimate resource for zoonoses is this book from the late Dr. David Schlossberg.
("My cat loves PPeanut BBuTTTer") #IDMedEd
Plague
Pasteurella
Bartonella
Bordetella bronchiseptica
Tularemia
Toxoplasma
Toxocara cati
Ultimate resource for zoonoses is this book from the late Dr. David Schlossberg.

2nd case presented at Grand Rounds today. The clues to the diagnosis are all in this famous Rembrandt painting. What’s your diagnosis? #IDMeded #IDgrandrounds #grandrounds @WashUID

Correct! This is the portrait of Gerard de Lairesse, displayed at the Metrop Museum of Art. Frontal bossing of Parrot, saddle nose, rhagades are just some of the many features of congenital syphilis depicted by Rembrandt. ncbi.nlm.nih.gov/pmc/articles/P…
The case presented today was a neonate who presented with fever, URI, and a diffuse discoid rash thought to be from neonatal lupus. RPR/TPA + so as mom’s. Cord blood negative (5% false negative RPR because of the Wharton Jelly within the umbilical cord).
