Discover and read the best of Twitter Threads about #IMPOCUS
Most recents (24)

ICU pictorials: A patient was admitted for "weakness". Unimpressive vitals / phys exam / labs. A few days later because of temp 101 F, a fever w/u was initiated. Due to "SOB", a CT chest angio was done:
👆Massive saddle PE extending in both sides w evidence of R heart strain 



Echo findings:

#POCUS quiz
1. What tracing did I obtain here?
2. What are some clinical scenarios where doing this would be helpful?
#IMPOCUS #MedEd #Nephpearls
1. What tracing did I obtain here?
2. What are some clinical scenarios where doing this would be helpful?
#IMPOCUS #MedEd #Nephpearls



ICU stories (a brief one): 60 yo male w lung cancer / CAD / HTN / HLD / status post chemotherapy a month ago presented to the ED w SOB/cough/weakness after failing outpatient tx w azithromycin. CT chest: no PE but positive for bilateral consolidations:
Patient came to the ICU intubated, sedated, on pressors & antibiotics for PNA. Next step: POCUS. PLAX looked "weird", so Doppler and "zoomed" views were recorded:
PSAX & subcostal views:
ICU stories (from the trenches): 70 yo pt w hx of A-fib/CAD/ICM w EF 25%/VT ablation s/p BiV ICD/CKD/HTN/HLD/peripheral vasc dz/COPD etc presented to outside 🏥 w SOB/weakness/falls. Labs: wbc 15k/creat 3.5 (baseline 2.0)/INR: 8.5/AST/ALT/Tbil: 180/250/3.0, lactate 3.5



RUQ US was obtained to work-up elevated LFTs:

Diagnosed w bilateral PNA/AKI/liver dysfunction. Treated for sepsis w ivf boluses, broad-spectrum antibiotics, steroids, bicarb. Continue to get worse; due to ⬆️O2 needs, transferred to our 🏥. I saw her the next am: in resp distress while on BiPAP 15/10-100%, abg 7.26/50/70/19.
ICU stories (a brief one): One hour before the end of the am shift, u walk around in the ICU to make sure thinks look OK before u type your sign-out note. You spot the resp therapist & the nurse bagging the pt in Rm 306. From the hallway, u see the monitor: HR 160, RR/45, Sat 70%
This is a 30 yo pt w hx of a catastrophic brain bleed, s/p trach & PEG, admitted 2 wks ago w MDR Klebsiella UTI. Doing well, on trach mask 28%, until the episode of acute/unexpected desaturation
When u examine the pt, s/he is in extremis (accessory muscle use-tachycardic-tachypneic-diaphoretic). BP: 105/55. You grab the stethoscope that the resp therapist wears around his neck & you hear breath sounds in both sides (pt is skinny...)
I just read this 👇 in the Comprehensive Critical Care: Adult, 3rd Edition; 2022 (@SCCM book). Are we still targeting CVP > 8?

ICU stories: 70 yo pt without medical hx but tobacco use (2 ppd x 40 y) was admitted w shortness of breath a wk ago. CXR/chest CT without PE/infiltrate. Was in afib/RVR on admission; placed on heparin & dilt/b-blocker (w some hypotension). Remained dyspneic, at times restless,
“requiring” multiple sedatives, & eventually was brought to the ICU. Intubated for "resp distress" & mental status changes. "Formal" echo, the day of ICU transfer, showed “LVEF 20% w global LV dysfunction”. On the vent 50% - peep 10. BP 110-130/60-70. Lactate < 2.0
Cards follow for "well compensated heart failure". A look w POCUS upon ICU admission:
How do you examine the lower extremity venous system when you look for deep vein thrombosis? What points do you check with the probe? Do you use Doppler? What are the recommended protocols? The Society of Radiologists in Ultrasound recommends a complete duplex ultrasound:

👆 The black rectangles represent the extent of the compression US. The gray rectangles are the sites of Doppler.
2-CUS (2-points compression US) includes compression of the femoral veins 1-2 cm above & below the saphenofemoral junction & the popliteal veins
up to the calf veins
2-CUS (2-points compression US) includes compression of the femoral veins 1-2 cm above & below the saphenofemoral junction & the popliteal veins
up to the calf veins
ECUS (extended compression US), includes compression US from the common femoral vein through the popliteal vein up to the calf veins confluence
CCUS (complete compression US), includes compression US from the common femoral vein to the ankle
CCUS (complete compression US), includes compression US from the common femoral vein to the ankle
ICU stories (a boring one…): If you work in a general ICU of a community hospital in United States, one of the common admissions you will get is the unfortunate resident of a nursing home or rehabilitation center that lives there for several decades & at some point becomes
febrile/“altered” & is sent to the ED for “evaluation”. The course is so predictable that we usually consider these admissions “boring”. This is the case of a middle-aged pt w cerebral palsy/mental retardation/seizures (on valproic)/PEG-chronic Foley in place who was sent to
the ED for fever+hypotension+tachycadia. Labs: WBC 15k, lactate 4.0. UA -as usually- suggestive of UTI (WBC>50, +bacteria, +nitrite, +esterase). CXR “clear” & pt w sat 99% on room air. Received ivf, Abx (pip/tazo + vanco) but due to persistent ⬇️BP, norepinephrine gtt was ordered
It's December, already. The time of the year when I am trying to spend every last cent of the annual allowance given to us for continuing medical education (CME) by our employer. In essence, this is money that we have worked for and, since it won't carry over to next year, I hate
leaving it on the table. The problem is that if you buy a conference or a study course now, you have to watch everything - and submit proof of attendance/completion - before the end of the year. So, it's a very busy month dedicated to studying/reviewing educational material!
For example, I just finished watching the last one of the 93 lectures from The Hospitalist & Resuscitationist 2022 conference #HR2022. If you are an intensivist/internist/family medicine/EM physician, I have no doubt that u will find several pearls to bring back to your practice
Head‑to‑toe #POCUS skills for intensivists in the general and neuro #intensivecareunit population: consensus and expert recommendations of the European Society of Intensive Care Medicine.
🔗pubmed.ncbi.nlm.nih.gov/34787687/
#MedEd #IMPOCUS
🔗pubmed.ncbi.nlm.nih.gov/34787687/
#MedEd #IMPOCUS


Thorax #POCUS

ICU stories: You get a call from outside 🏥 to accept a middle-aged pt w DM2/HTN/HLD/some type of solid Ca on chemo/obesity who presented to their ED w weakness/anxiety/"feeling cold". Vitals: BP 80-100, HR 130s (sinus tach), afebrile, Sat 100% on room air. Labs: WBC 13K, ...
... Lactate 5.2, creat 1.3. UA w some WBCs/bacteria. CXR clear. Norepi drip ordered but cancelled after BP improved to mid-90s, HR fell to 120s, & lactate ⬇️ to 2.5. What's your next step?
The discussion went like this:
Me: I will be happy to accept but I have no idea what we are treating. If it is sepsis, the source is unclear. And what about PE? Can you pls get a CT before sending?
ED: Sure, will do it. Thanks.
You go home & next am you learn that the CT showed:
Me: I will be happy to accept but I have no idea what we are treating. If it is sepsis, the source is unclear. And what about PE? Can you pls get a CT before sending?
ED: Sure, will do it. Thanks.
You go home & next am you learn that the CT showed:
RV enlargement for #POCUS purposes: In the apical 4-chamber view, if the RV is slightly bigger than the normal configuration of 1/3 - 2/3, its mild enlargement, RV = LV is moderate, RV > LV is severe.
#IMPOCUS #MedEd #Nephrology
#IMPOCUS #MedEd #Nephrology



A short 🧵 on hepatic vein #VExUS and key pathologies
From: jacc.org/doi/10.1016/j.…
1/ HV Anatomy & Normal Flow Profile, respiratory variation (forward flow [S,D] ⬆️ during inspiration)
Click ‘ALT’ for normal waveform description
#POCUS #MedEd #Nephrology #IMPOCUS #FOAMed
From: jacc.org/doi/10.1016/j.…
1/ HV Anatomy & Normal Flow Profile, respiratory variation (forward flow [S,D] ⬆️ during inspiration)
Click ‘ALT’ for normal waveform description
#POCUS #MedEd #Nephrology #IMPOCUS #FOAMed

2/ A. Tricuspid regurgitation: Systolic flow reversal
B. Tricuspid stenosis: prolonged deceleration time of the D-wave + prominent A-wave
Click ‘ALT’ for further description
#POCUS #VExUS
B. Tricuspid stenosis: prolonged deceleration time of the D-wave + prominent A-wave
Click ‘ALT’ for further description
#POCUS #VExUS

A. Constrictive pericarditis: expiratory ⬇️ in tricuspid flow & RV filling with associated flow reversals on HVD
B. Restrictive cardiomyopathy: prominent D reversals during inspiration
C. ⬆️RVEDP: prominent A-wave
D. RV systolic dysfunction: ⬇️ S-wave
‘ALT’ for description (A&B)
B. Restrictive cardiomyopathy: prominent D reversals during inspiration
C. ⬆️RVEDP: prominent A-wave
D. RV systolic dysfunction: ⬇️ S-wave
‘ALT’ for description (A&B)
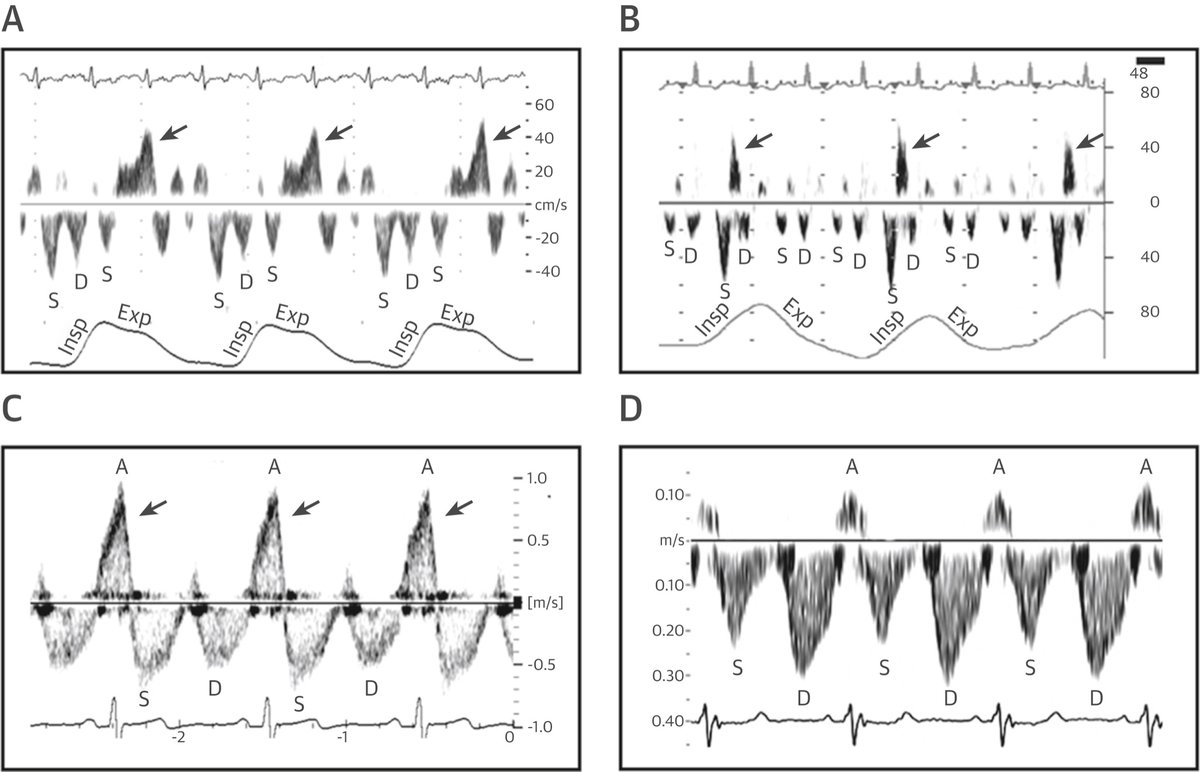
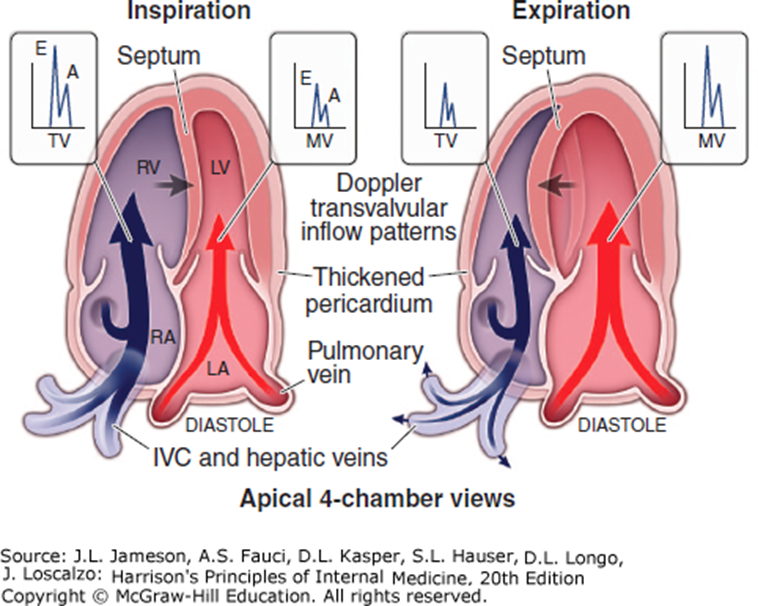
Illustration of the Effects of Changes in Intrathoracic and Intracardiac Pressures During Respiration in Normal Versus Constrictive Heart.
#echofirst #MedEd #POCUS #IMPOCUS
🔗 sciencedirect.com/science/articl…
#echofirst #MedEd #POCUS #IMPOCUS
🔗 sciencedirect.com/science/articl…

Typical changes during respiration in the interventricular septum movement (white arrows) and blood flow velocities (black arrows). Insets depict typical Doppler velocity (y-axis) versus time (x-axis) tracings across
MV, TV, PV & HV.
🔗nature.com/articles/nrcar…
#POCUS #echofirst
MV, TV, PV & HV.
🔗nature.com/articles/nrcar…
#POCUS #echofirst

Another easy-to-understand representation of variation on transmitral and tricuspid flow in constrictive pericarditis.
ICU POCUS snippets: A bit of context: An elderly patient with hx of DM2 / HTN / HLD / peripheral vascular disease / ureteral stent & recurrent UTIs is admitted to the hospitalists’ service w diffuse abdominal pain, nausea & vomiting. Treated for a few days w antibiotics...
...but never really felt any better (weak/abd pain). Eventually, became hypotensive & was transferred to the ICU for “initiation of vasopressors”. Phys exam: diffuse abd tenderness. Formal echo earlier that day: "Normal LV/RV in size and systolic function". ICU POCUS was done...
...to gain more information regarding the cause of the abd pain and the hemodynamic picture. Some of the clips are shown here:
Cardiac tamponade on #POCUS #echofirst
Click on 'ALT' for description
#MedEd #IMPOCUS #Nephrology
From 🔗pubmed.ncbi.nlm.nih.gov/32572594/
Click on 'ALT' for description
#MedEd #IMPOCUS #Nephrology
From 🔗pubmed.ncbi.nlm.nih.gov/32572594/


Pulsus paradoxus: during inspiration, right heart filling occurs at the expense of the left, so that its transmural pressure transiently improves & then reverts during expiration (Ventricular interdependence). Seen as 👆on #POCUS

ICU POCUS snippets: Much has been said about how useful lung POCUS is for procedural guidance. First of all, it accurately reveals large effusions when the radiology report characterizes them as “small”. This is from a recent case of a pt intubated w community-acquired pneumonia

and what proved to be bilateral parapneumonic effusions:
Secondly, while the dogma (which, btw, I don’t recommend completely ignoring!) in thoracentesis is to insert the needle at the “triangle of safety”, bordered by the anterior border of the latissimus dorsi, the lateral border of the pectoralis major, the horizontal line at the...
One of my favorite topics in #POCUS - various effusions seen from different sonographic windows.
Here is a thread 🧵with labeled images for those interested.
1. PLAX view - pericardial effusion - anterior to descending aorta ⚫️below LA), wedge shaped
#MedEd #IMPOCUS #Nephpearls
Here is a thread 🧵with labeled images for those interested.
1. PLAX view - pericardial effusion - anterior to descending aorta ⚫️below LA), wedge shaped
#MedEd #IMPOCUS #Nephpearls
2/ PSAX papillary muscle view
LV is think as many of my patients have #CKD and LVH (as well as mitral annular calcification seen on PLAX view above)
#Nephrology #POCUS
LV is think as many of my patients have #CKD and LVH (as well as mitral annular calcification seen on PLAX view above)
#Nephrology #POCUS
3/ Apical 4-chamber view
Sometimes, effusions may be missed due to inadequate visualization of ventricular free wall/lung interference. Always pay attention to the RA area
#POCUS
Sometimes, effusions may be missed due to inadequate visualization of ventricular free wall/lung interference. Always pay attention to the RA area
#POCUS
Small thread 🧵illustrating #POCUS based hemodynamic assessment. Relatively a classic case of pulmonary HTN and right heart failure but would like to get some insights from the experts.
1/ Parasternal long axis (PSAX) showing D-sign
#VExUS #MedEd #Nephpearls #IMPOCUS
1/ Parasternal long axis (PSAX) showing D-sign
#VExUS #MedEd #Nephpearls #IMPOCUS
2/ Parasternal long axis (PLAX) view demonstrating RV dilatation.
One of the three musketeers is big. Don't know what I'm talking about? Here is a brief reminder: 🔗nephropocus.com/2021/07/12/the…
(Mobile thing in the RVOT is PA catheter; M-mode quiz from this morning is actually this)
One of the three musketeers is big. Don't know what I'm talking about? Here is a brief reminder: 🔗nephropocus.com/2021/07/12/the…
(Mobile thing in the RVOT is PA catheter; M-mode quiz from this morning is actually this)
3/ Apical 4-chamber view #POCUS
Note how RV is dilated - bigger than LV and forming the cardiac apex.
Inter-atrial septum is bowing to the left indicating high right atrial pressure (not unexpected).
Note how RV is dilated - bigger than LV and forming the cardiac apex.
Inter-atrial septum is bowing to the left indicating high right atrial pressure (not unexpected).

S/P MVC c Rt CP/SOB- 118/74, 112, 24, 96% RA. Supine pCXR. #FOAMed #FOAMcc #MedEd #MedTwitter #EMBound #Impocus #POCUS #FOAMus @msiuba @siddharth_dugar @ThinkingCC @khaycock2 @pdsalinas @msenussiMD @IM_Crit_ @KalagaraHari @iceman_ex @NephroP @EM_RESUS @jminardi21 @TomJelic

Management? @kyliebaker888 @medpedshosp @dan___kim @TaotePOCUS @Manoj_Wickram @ria_dancel @SmallsSono @drjgutt @medcramUS @POCUSaurusRex @PratsEM @HeyDrNik @MH_EMultrasound @MetroHealth_EM
Management if patient was tachypneic/hypotensive based on CXR?

Humbling pleural procedure case to share.
70 y/o admitted with fever, hypoxia, R flank pain, loculated pleural effusion (right lower) on CXR. Concern for empyema prompting abx, chest US and possible intervention.
How would you manage? (poll to follow)
#POCUS #IMPOCUS
1/
70 y/o admitted with fever, hypoxia, R flank pain, loculated pleural effusion (right lower) on CXR. Concern for empyema prompting abx, chest US and possible intervention.
How would you manage? (poll to follow)
#POCUS #IMPOCUS
1/
2/
It is overnight on the ward. Which of the following would be your advised management?
3/
3/
ICU stories: Middle-aged pt w PMHx of rheum fever/A fib underwent MV+AV replacement, TV repair w ring, Maze procedure + LA appendage closure. At the end of surgery, TEE was “fine”; pt was transferred to the ICU intubated (fio2 40%) on low-dose levo (0.04). Could not be extubated
because few h later, lactate began to ⬆️ and ivf were given. Levo gtt did not ⬆️ much (just @ 0.1 next am) but lactate was up to 17 mmol/l & pH was 6.98. I was told that pt was probably still "under-resuscitated". When I 👀the chart, pt had received multiple NS, bicarb & albumin
boluses and was > 8 liters positive. I first pulled the bed sheets to look at the legs and feel the skin temp:

